

Real-Time Microscope-Integrated OCT to Improve Visualization in DSAEK for Advanced Bullous Keratopathy
- PMID: 26509766
- PMCID: PMC4636956
- DOI: 10.1097/ICO.0000000000000661
Real-Time Microscope-Integrated OCT to Improve Visualization in DSAEK for Advanced Bullous Keratopathy
Abstract
Purpose: To report the intraoperative use of microscope-integrated optical coherence tomography (MIOCT) to enable visualization for Descemet's stripping automated endothelial keratoplasty (DSAEK) in 2 patients with advanced bullous keratopathy.
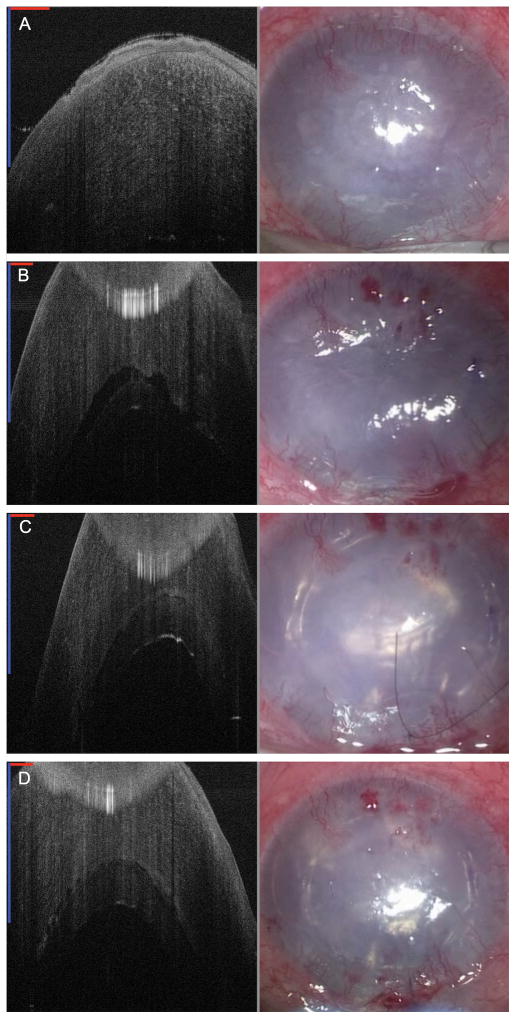
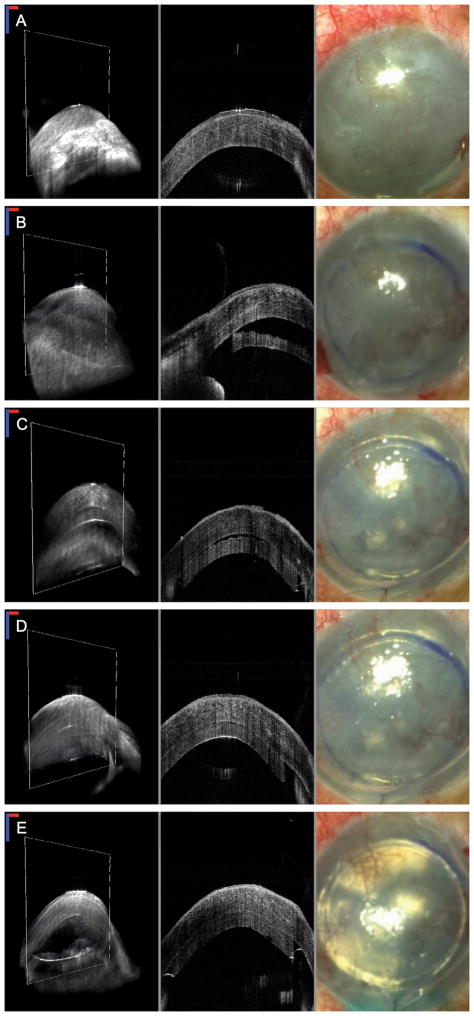
Methods: Patient 1 was an 83-year-old female and patient 2 was a 28-year-old male both with limited vision and significant pain from bullous keratopathy who underwent palliative DSAEK. Because of the severity and chronicity of the corneal decompensation in both patients, the view past the anterior cornea was negligible using standard microscope illumination techniques. We used spectral-domain (Patient 1) and swept-source (Patient 2) MIOCT, both of which rely on infrared illumination, to visualize key parts of the DSAEK procedure.
Results: Graft insertion, unfolding, tamponade, and attachment could be dynamically visualized intraoperatively despite the nearly opaque nature of the host corneas. Postoperatively, the grafts remained attached with significant corneal clearing, and there was improvement in visual acuity, and pain relief for both patients.
Conclusions: MIOCT is a valuable tool for the corneal surgeon, allowing for DSAEK to be successfully performed even when the surgical microscope view is limited from severe corneal edema, as is often the case in patients with advanced bullous keratopathy. By using MIOCT, these patients can benefit from the advantages of DSAEK despite a clinically opaque cornea, which would otherwise be treated with a penetrating keratoplasty.
Trial registration: ClinicalTrials.gov NCT01588041.
Conflict of interest statement
At the time of this work, Dr. Izatt was Chairman and Chief Scientific Advisor for Bioptigen, Inc., and had corporate, equity, and intellectual property interests (including royalties) in this company.
Dr. Toth receives financial support from Alcon, Bioptigen, and Genentech, is a consultant to Thrombogenics, and has an intraoperative imaging patent with Duke University. Dr. Kuo has an imaging algorithm patent licensed by Duke to Bioptigen. For the remaining authors no conflicts were declared.
Figures
References
-
- Bahar I, Kaiserman I, Levinger E, et al. Retrospective contralateral study comparing descemet stripping automated endothelial keratoplasty with penetrating keratoplasty. Cornea. 2009;28:485–8. - PubMed
-
- Hjortdal J, Pedersen IB, Bak-Nielsen S, et al. Graft rejection and graft failure after penetrating keratoplasty or posterior lamellar keratoplasty for fuchs endothelial dystrophy. Cornea. 2013;32:e60–3. - PubMed
-
- Li JY, Terry MA, Goshe J, et al. Three-year visual acuity outcomes after Descemet’s stripping automated endothelial keratoplasty. Ophthalmology. 2012;119:1126–9. - PubMed
-
- Ratanasit A, Gorovoy MS. Long-term results of Descemet stripping automated endothelial keratoplasty. Cornea. 2011;30:1414–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
