

Local Control Rates of Metastatic Renal Cell Carcinoma (RCC) to Thoracic, Abdominal, and Soft Tissue Lesions Using Stereotactic Body Radiotherapy (SBRT)
- PMID: 26510665
- PMCID: PMC4625576
- DOI: 10.1186/s13014-015-0528-z
Local Control Rates of Metastatic Renal Cell Carcinoma (RCC) to Thoracic, Abdominal, and Soft Tissue Lesions Using Stereotactic Body Radiotherapy (SBRT)
Abstract
Background and purpose: We report the radiographic response rate of SBRT compared to conventional fractionated radiotherapy (CF-EBRT) for thoracic, abdominal, skin and soft tissue RCC lesions treated at our institution.
Material and methods: Fifty three lesions where included in the study (36 SBRT, 17 CF-EBRT), treated from 2004 to 2014 at our institution. We included patients that had thoracic, skin & soft tissue (SST), and abdominal metastases of histologically confirmed RCC. The most common SBRT fractionation was 50 Gy in 5 fractions.
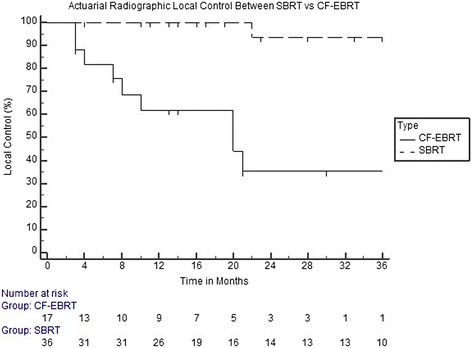
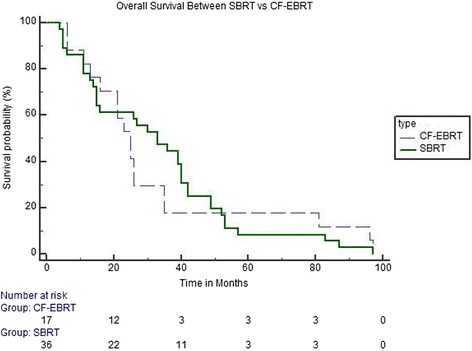
Results: The median time of follow-up was 16 months (range 3-97 months). Median BED was 216.67 (range 66.67-460.0) for SBRT, and 60 (range 46.67-100.83) for CF-EBRT. Median radiographic local control rates at 12, 24, and 36 months were 100, 93.41, and 93.41 % for lesions treated with SBRT versus 62.02, 35.27 and 35.27 % for those treated with CF-EBRT (p < 0.001). Predictive factors for radiographic local control under univariate analysis included BED ≥ 100 Gy (HR, 0.048; 95 % CI, 0.006-0.382; p = 0.005), dose per fraction ≥ 9 Gy (HR, 0.631; 95 % CI, 0.429-0.931; p = 0.021), and gender (HR, 0.254; 95 % CI, 0.066-0.978; p = 0.048). Under multivariate analysis, there were no significant predictors for local control. Toxicity rates were low and equivalent in both groups, with no grade 4 or 5 side effects reported.
Conclusions: SBRT is safe and effective for the treatment of RCC metastases to thoracic, abdominal and integumentary soft tissues. Radiographic response rates were greater and more durable using SBRT compared to CF-EBRT. Further prospective trials are needed to evaluate efficacy and safety of SBRT for RCC metastases.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
