

The contribution of the anaesthetist to risk-adjusted mortality after cardiac surgery
- PMID: 26511481
- PMCID: PMC4949638
- DOI: 10.1111/anae.13291
The contribution of the anaesthetist to risk-adjusted mortality after cardiac surgery
Abstract
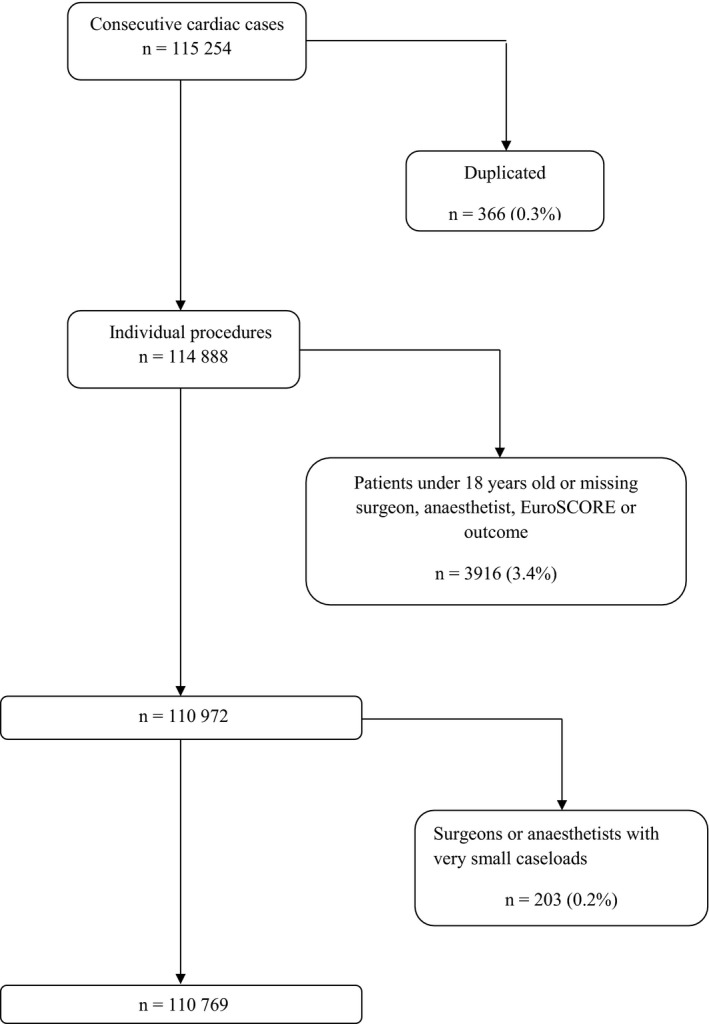
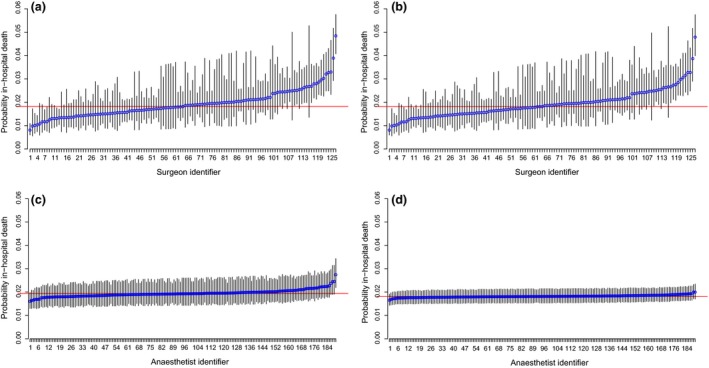
It is widely accepted that the performance of the operating surgeon affects outcomes, and this has led to the publication of surgical results in the public domain. However, the effect of other members of the multidisciplinary team is unknown. We studied the effect of the anaesthetist on mortality after cardiac surgery by analysing data collected prospectively over ten years of consecutive cardiac surgical cases from ten UK centres. Casemix-adjusted outcomes were analysed in models that included random-effects for centre, surgeon and anaesthetist. All cardiac surgical operations for which the EuroSCORE model is appropriate were included, and the primary outcome was in-hospital death up to three months postoperatively. A total of 110 769 cardiac surgical procedures conducted between April 2002 and March 2012 were studied, which included 127 consultant surgeons and 190 consultant anaesthetists. The overwhelming factor associated with outcome was patient risk, accounting for 95.75% of the variation for in-hospital mortality. The impact of the surgeon was moderate (intra-class correlation coefficient 4.00% for mortality), and the impact of the anaesthetist was negligible (0.25%). There was no significant effect of anaesthetist volume above ten cases per year. We conclude that mortality after cardiac surgery is primarily determined by the patient, with small but significant differences between surgeons. Anaesthetists did not appear to affect mortality. These findings do not support public disclosure of cardiac anaesthetists' results, but substantially validate current UK cardiac anaesthetic training and practice. Further research is required to establish the potential effects of very low anaesthetic caseloads and the effect of cardiac anaesthetists on patient morbidity.
© 2015 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists of Great Britain and Ireland.
Figures
Comment in
-
Asked and answered: is the mortality associated with cardiac surgery related to the anaesthetist and should it be used to measure anaesthetic performance?Anaesthesia. 2016 Feb;71(2):123-6. doi: 10.1111/anae.13315. Epub 2015 Oct 28. Anaesthesia. 2016. PMID: 26511619 No abstract available.
-
Death after cardiac surgery is chiefly due to patient risk factors, study finds.BMJ. 2015 Nov 1;351:h5821. doi: 10.1136/bmj.h5821. BMJ. 2015. PMID: 26525062 No abstract available.
-
Publishing anaesthetists' clinical outcomes.Anaesthesia. 2016 May;71(5):596-7. doi: 10.1111/anae.13437. Anaesthesia. 2016. PMID: 27072764 No abstract available.
-
Anaesthetists' contribution to mortality after cardiac surgery.Anaesthesia. 2016 May;71(5):597-8. doi: 10.1111/anae.13474. Anaesthesia. 2016. PMID: 27072765 No abstract available.
-
Transoesophageal echocardiography skills.Anaesthesia. 2016 May;71(5):598. doi: 10.1111/anae.13457. Anaesthesia. 2016. PMID: 27072766 No abstract available.
-
Anaesthetist contribution to mortality after cardiac surgery - a reply.Anaesthesia. 2016 May;71(5):599-601. doi: 10.1111/anae.13475. Anaesthesia. 2016. PMID: 27072767 No abstract available.
-
Climate change in cardiothoracic intensive care.Anaesthesia. 2016 Dec;71(12):1395-1398. doi: 10.1111/anae.13646. Epub 2016 Sep 26. Anaesthesia. 2016. PMID: 27666428 No abstract available.
References
-
- Neumayer L. Design and conduct issues in surgical clinical trials. American Journal of Surgery 2004; 188: 17S–21S. - PubMed
-
- Campbell MK, Piaggio G, Elbourne DR, Altman DG; the CONSORT group . Consort 2010 statement: extension to cluster radomised trials. British Medical Journal 2012; 345: e5661. - PubMed
-
- McCulloch P, Altman DG, Campbell WB, et al.; for the Balliol Collaboration . No surgical innovation without evaluation: the IDEAL recommendations. Lancet 2009; 374: 1105–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
