

The gut microbiota plays a protective role in the host defence against pneumococcal pneumonia
- PMID: 26511795
- PMCID: PMC4819612
- DOI: 10.1136/gutjnl-2015-309728
The gut microbiota plays a protective role in the host defence against pneumococcal pneumonia
Abstract
Objective: Pneumonia accounts for more deaths than any other infectious disease worldwide. The intestinal microbiota supports local mucosal immunity and is increasingly recognised as an important modulator of the systemic immune system. The precise role of the gut microbiota in bacterial pneumonia, however, is unknown. Here, we investigate the function of the gut microbiota in the host defence against Streptococcus pneumoniae infections.
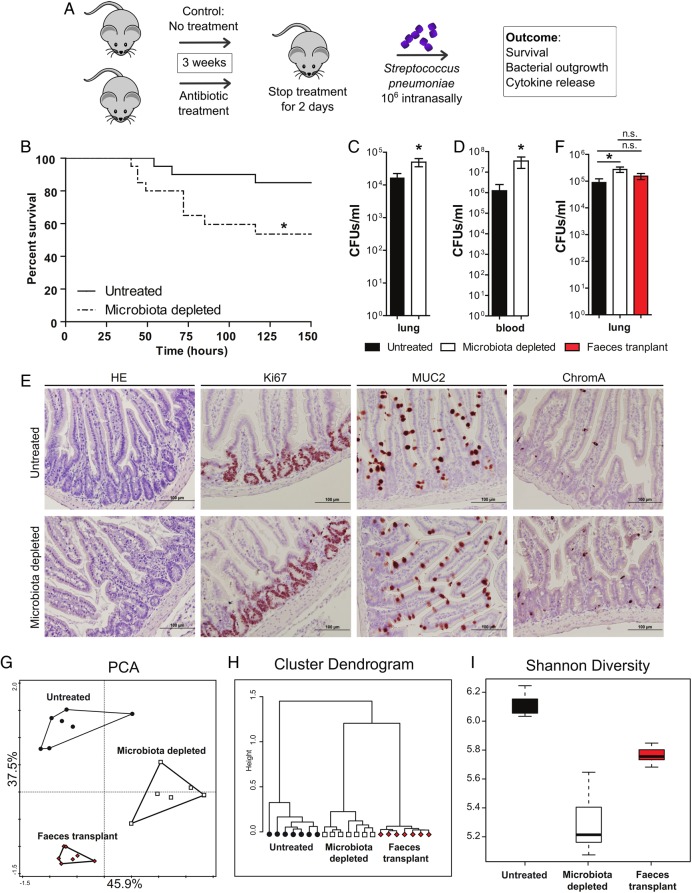
Design: We depleted the gut microbiota in C57BL/6 mice and subsequently infected them intranasally with S. pneumoniae. We then performed survival and faecal microbiota transplantation (FMT) experiments and measured parameters of inflammation and alveolar macrophage whole-genome responses.
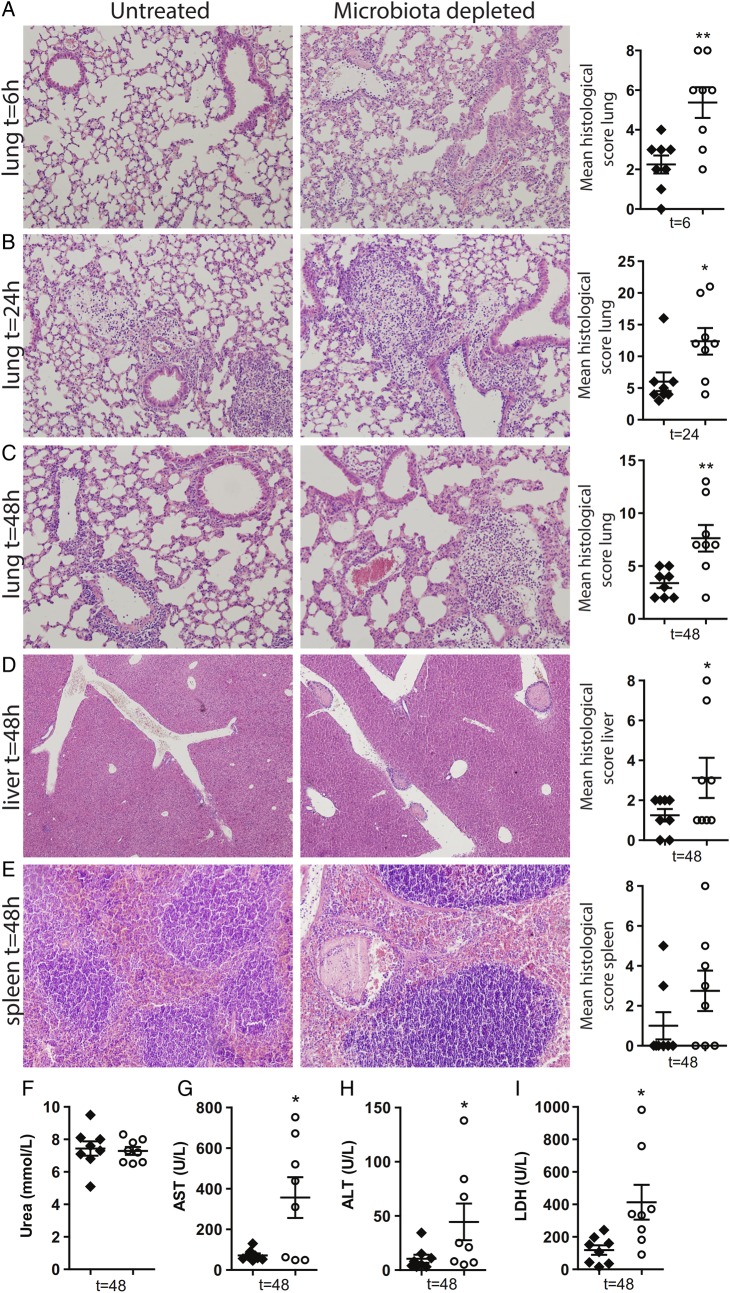
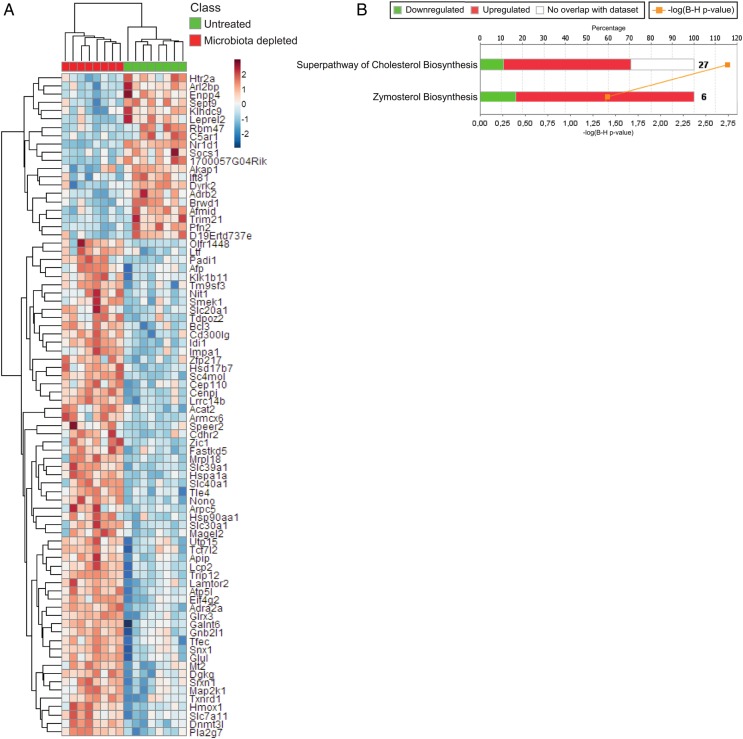
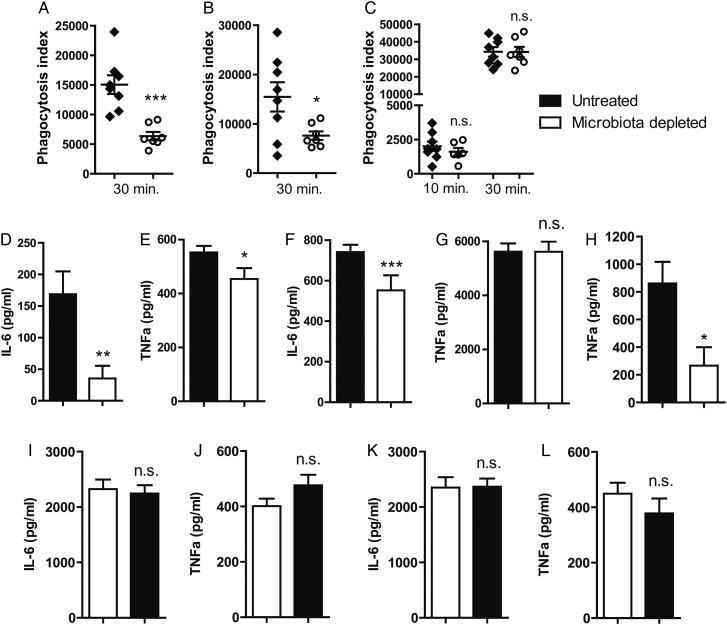
Results: We found that the gut microbiota protects the host during pneumococcal pneumonia, as reflected by increased bacterial dissemination, inflammation, organ damage and mortality in microbiota-depleted mice compared with controls. FMT in gut microbiota-depleted mice led to a normalisation of pulmonary bacterial counts and tumour necrosis factor-α and interleukin-10 levels 6 h after pneumococcal infection. Whole-genome mapping of alveolar macrophages showed upregulation of metabolic pathways in the absence of a healthy gut microbiota. This upregulation correlated with an altered cellular responsiveness, reflected by a reduced responsiveness to lipopolysaccharide and lipoteichoic acid. Compared with controls, alveolar macrophages derived from gut microbiota-depleted mice showed a diminished capacity to phagocytose S. pneumoniae.
Conclusions: This study identifies the intestinal microbiota as a protective mediator during pneumococcal pneumonia. The gut microbiota enhances primary alveolar macrophage function. Novel therapeutic strategies could exploit the gut-lung axis in bacterial infections.
Keywords: BACTERIAL INFECTION; BACTERIAL PATHOGENESIS; IMMUNOLOGY; INTESTINAL MICROBIOLOGY; SEPSIS.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
Comment in
-
Gut microbiota and protection from pneumococcal pneumonia.Gut. 2017 Feb;66(2):384. doi: 10.1136/gutjnl-2016-311823. Epub 2016 Apr 1. Gut. 2017. PMID: 27037327 Free PMC article. No abstract available.
-
Reply to letter to the editor of Gut by Dickson and Cox.Gut. 2017 Mar;66(3):556. doi: 10.1136/gutjnl-2016-311910. Epub 2016 Apr 15. Gut. 2017. PMID: 27196575 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources