

Normal Development and Measurements of the Occipital Condyle-C1 Interval in Children and Young Adults
- PMID: 26514612
- PMCID: PMC7960296
- DOI: 10.3174/ajnr.A4543
Normal Development and Measurements of the Occipital Condyle-C1 Interval in Children and Young Adults
Abstract
Background and purpose: Widening of the occipital condyle-C1 interval is the most specific and sensitive means of detecting atlanto-occipital dislocation. Recent studies attempting to define normal measurements of the condyle-C1 interval in children have varied substantially. This study was performed to test the null hypothesis that condyle-C1 interval morphology and joint measurements do not change as a function of age.
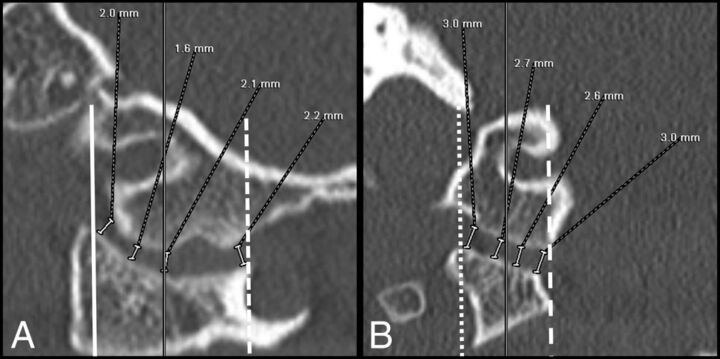
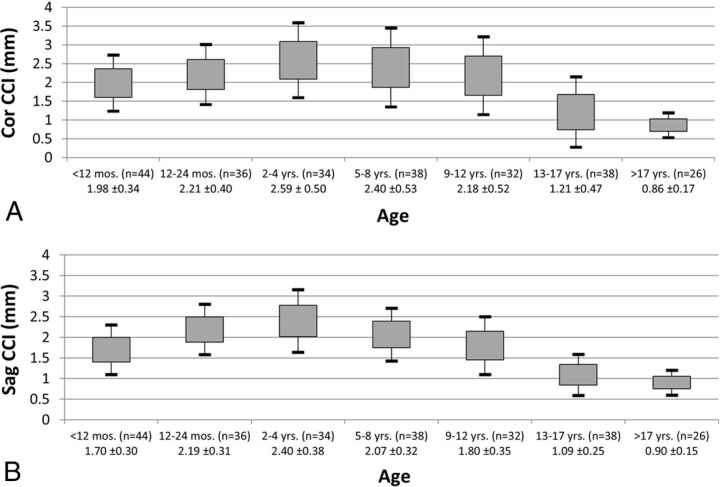
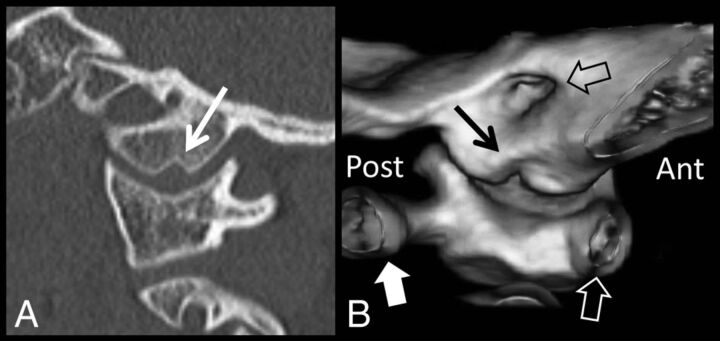
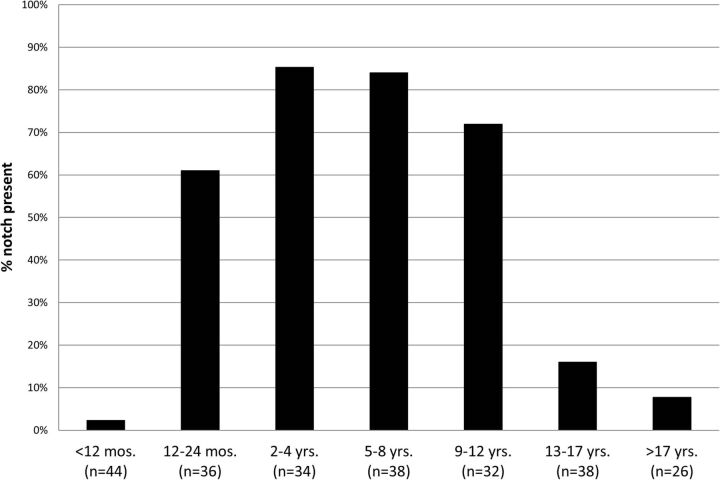
Materials and methods: Imaging review of subjects undergoing CT of the upper cervical spine for reasons unrelated to trauma or developmental abnormality was performed. Four equidistant measurements were obtained for each bilateral condyle-C1 interval on sagittal and coronal images. The cohort was divided into 7 age groups to calculate the mean, SD, and 95% CIs for the average condyle-C1 interval in both planes. The prevalence of a medial occipital condyle notch was calculated.
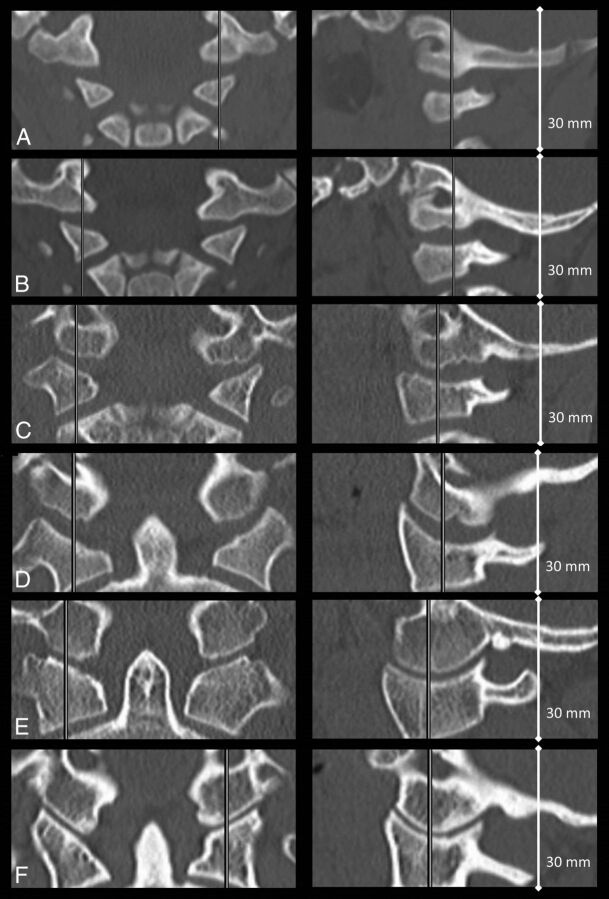
Results: Two hundred forty-eight joints were measured in 124 subjects with an age range of 2 days to 22 years. The condyle-C1 interval varies substantially by age. Average coronal measurements are larger and more variable than sagittal measurements. The medial occipital condyle notch is most prevalent from 1 to 12 years and is uncommon in older adolescents and young adults.
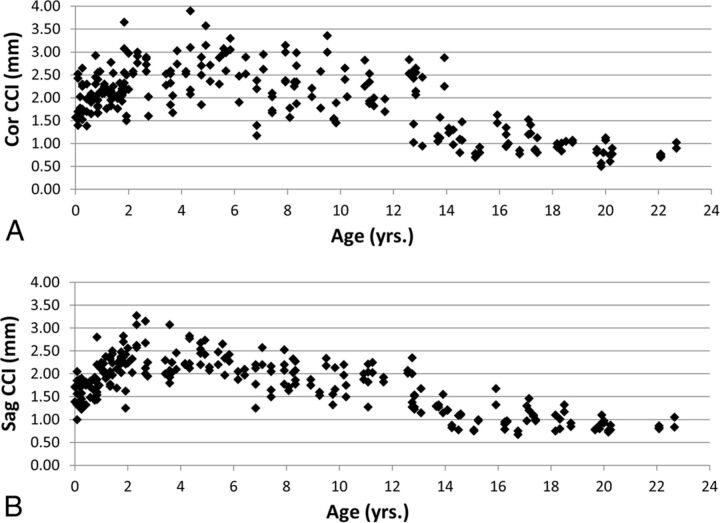
Conclusions: The condyle-C1 interval increases during the first several years of life, is largest in the 2- to 4-year age range, and then decreases through late childhood and adolescence. A single threshold value to detect atlanto-occipital dissociation may not be sensitive and specific for all age groups. Application of this normative data to documented cases of atlanto-occipital injury is needed to determine clinical utility.
© 2016 by American Journal of Neuroradiology.
Figures
References
-
- Pang D, Nemzek WR, Zovickian J. Atlanto-occipital dislocation, part 2: the clinical use of (occipital) condyle-C1 interval, comparison with other diagnostic methods, and the manifestation, management, and outcome of atlanto-occipital dislocation in children. Neurosurgery 2007;61:995–1015; discussion 1015 10.1227/01.neu.0000303196.87672.78 - DOI - PubMed
-
- Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development of the Hand and Wrist. Stanford: Stanford University Press; 1959
MeSH terms
LinkOut - more resources
Full Text Sources