

Adverse pregnancy outcomes in rural Uganda (1996-2013): trends and associated factors from serial cross sectional surveys
- PMID: 26515763
- PMCID: PMC4627380
- DOI: 10.1186/s12884-015-0708-8
Adverse pregnancy outcomes in rural Uganda (1996-2013): trends and associated factors from serial cross sectional surveys
Abstract
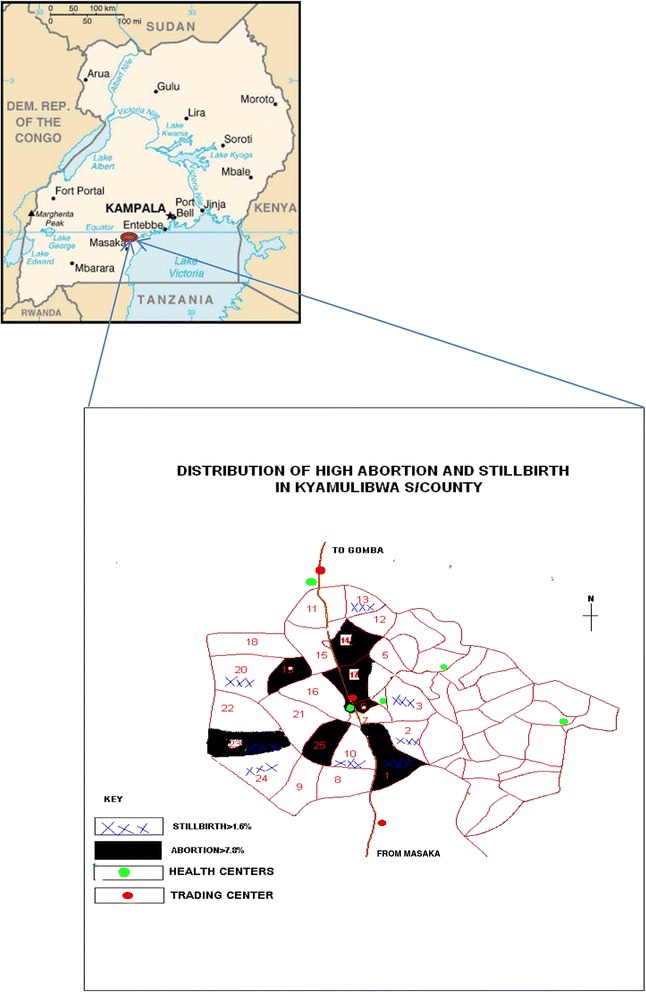
Objective: Community based evidence on pregnancy outcomes in rural Africa is lacking yet it is needed to guide maternal and child health interventions. We estimated and compared adverse pregnancy outcomes and associated factors in rural south-western Uganda using two survey methods.
Methods: Within a general population cohort, between 1996 and 2013, women aged 15-49 years were interviewed on their pregnancy outcome in the past 12 months (method 1). During 2012-13, women in the same cohort were interviewed on their lifetime experience of pregnancy outcomes (method 2). Adverse pregnancy outcome was defined as abortions or stillbirths. We used random effects logistic regression for method 1 and negative binomial regression with robust clustered standard errors for method 2 to explore factors associated with adverse outcome.
Results: One third of women reported an adverse pregnancy outcome; 10.8% (abortion = 8.4%, stillbirth = 2.4%) by method 1 and 8.5% (abortion = 7.2%, stillbirth = 1.3%) by method 2. Abortion rates were similar (10.8 vs 10.5) per 1000 women and stillbirth rates differed (26.2 vs 13.8) per 1000 births by methods 1 and 2 respectively. Abortion risk increased with age of mother, non-attendance of antenatal care and proximity to the road. Lifetime stillbirth risk increased with age. Abortion and stillbirth risk reduced with increasing parity.
Discussion: Both methods had a high level of agreement in estimating abortion rate but were markedly below national estimates. Stillbirth rate estimated by method 1 was double that estimated by method 2 but method 1 estimate was more consistent with the national estimates.
Conclusion: Strategies to improve prospective community level data collection to reduce reporting biases are needed to guide maternal health interventions.
Figures
References
-
- UNICEF . United nations department for economic and social information and policy analysis. World population prospects: the 2008 revision. New York: United Nations; 2009.
-
- Singh S, Wulf D, Hussain R, Bankole A, Sedgh G. Abortion worldwide: a decade of uneven progress. Guttmacher Institute, New York, USA. 2009
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
