

Synergistic Effects of Combined Cell Therapy for Chronic Ischemic Cardiomyopathy
- PMID: 26516002
- PMCID: PMC4628729
- DOI: 10.1016/j.jacc.2015.08.879
Synergistic Effects of Combined Cell Therapy for Chronic Ischemic Cardiomyopathy
Abstract
Background: Both bone marrow-derived mesenchymal stem cells (MSCs) and c-kit(+) cardiac stem cells (CSCs) improve left ventricular remodeling in porcine models and clinical trials. Using xenogeneic (human) cells in immunosuppressed animals with acute ischemic heart disease, we previously showed that these 2 cell types act synergistically.
Objectives: To more accurately model clinical applications for heart failure, this study tested whether the combination of autologous MSCs and CSCs produce greater improvement in cardiac performance than MSCs alone in a nonimmunosuppressed porcine model of chronic ischemic cardiomyopathy.
Methods: Three months after ischemia/reperfusion injury, Göttingen swine received transendocardial injections with MSCs alone (n = 6) or in combination with cardiac-derived CSCs (n = 8), or placebo (vehicle; n = 6). Cardiac functional and anatomic parameters were assessed using cardiac magnetic resonance at baseline and before and after therapy.
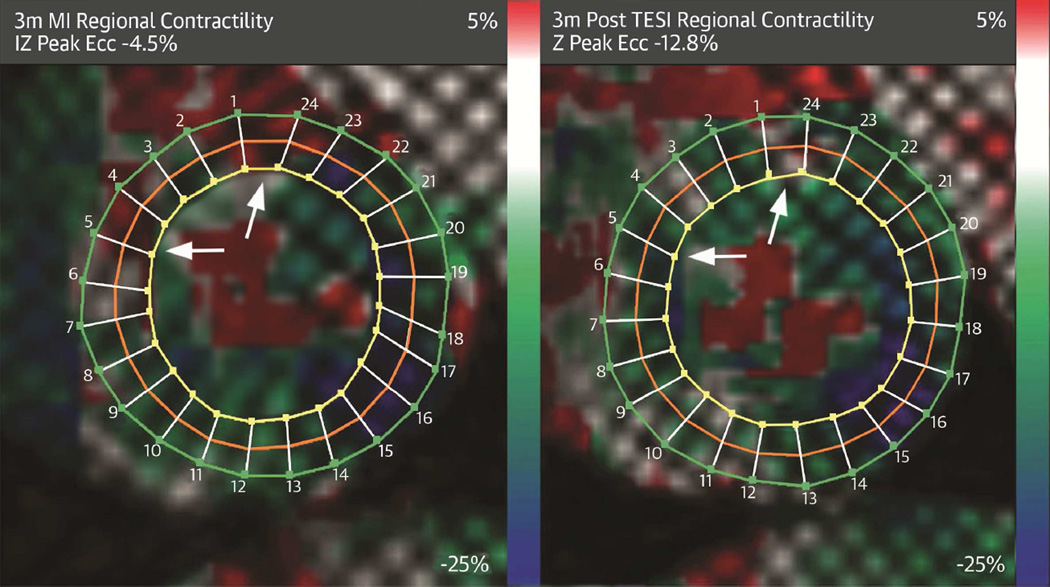
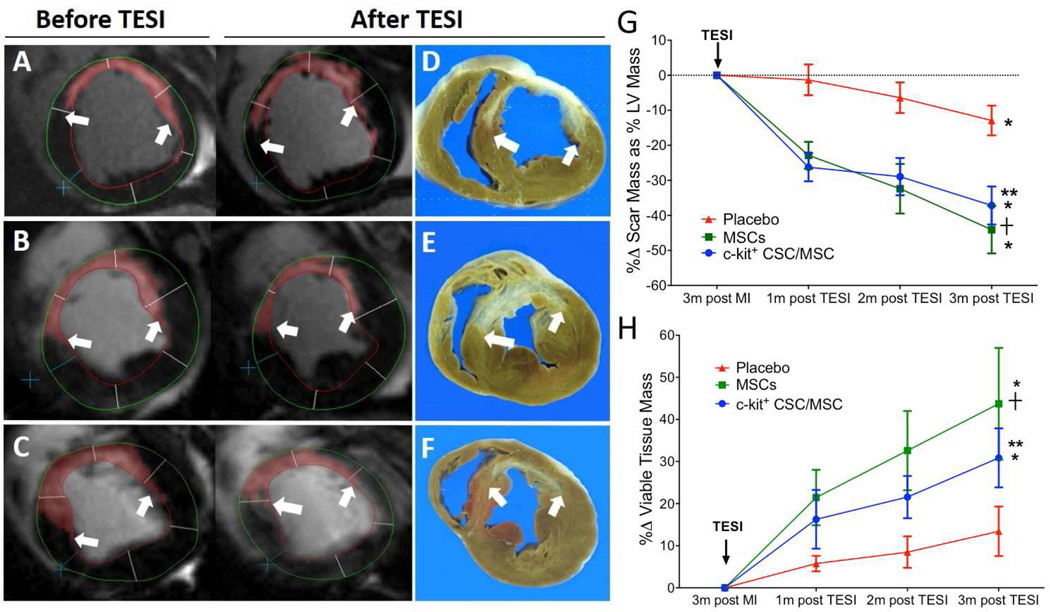
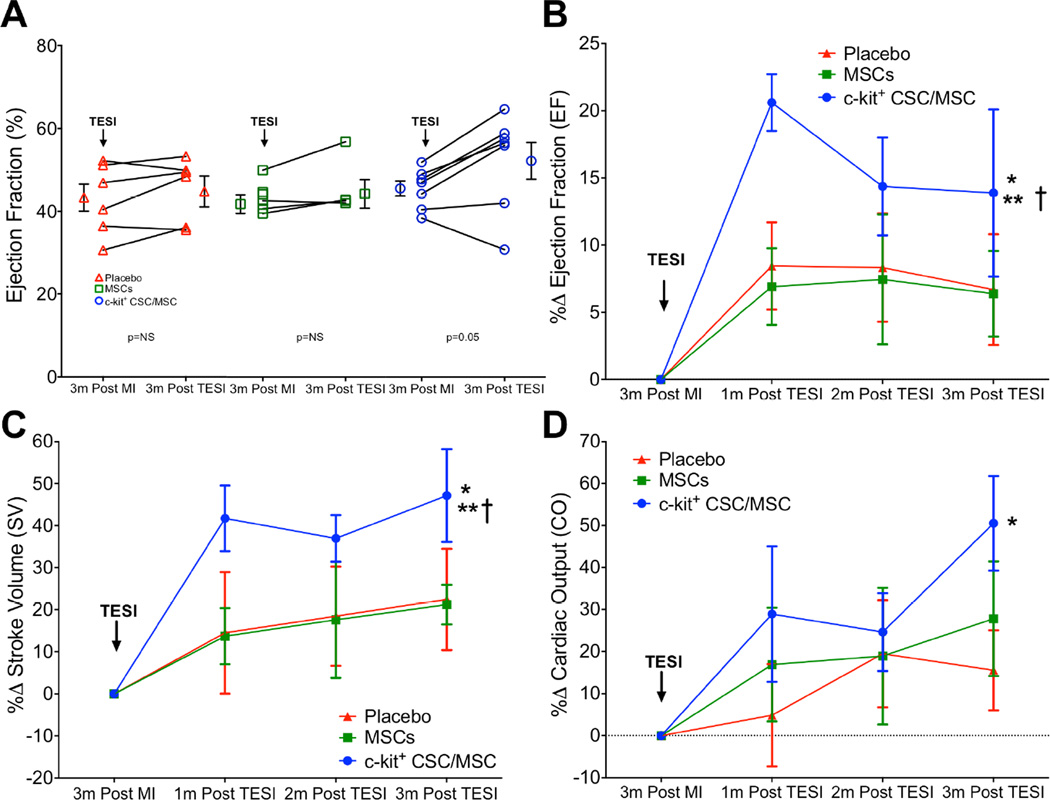
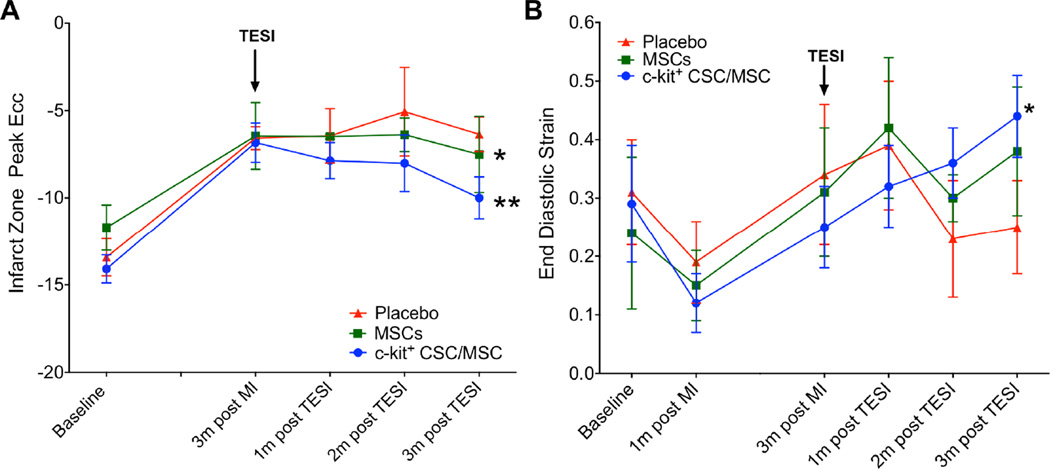
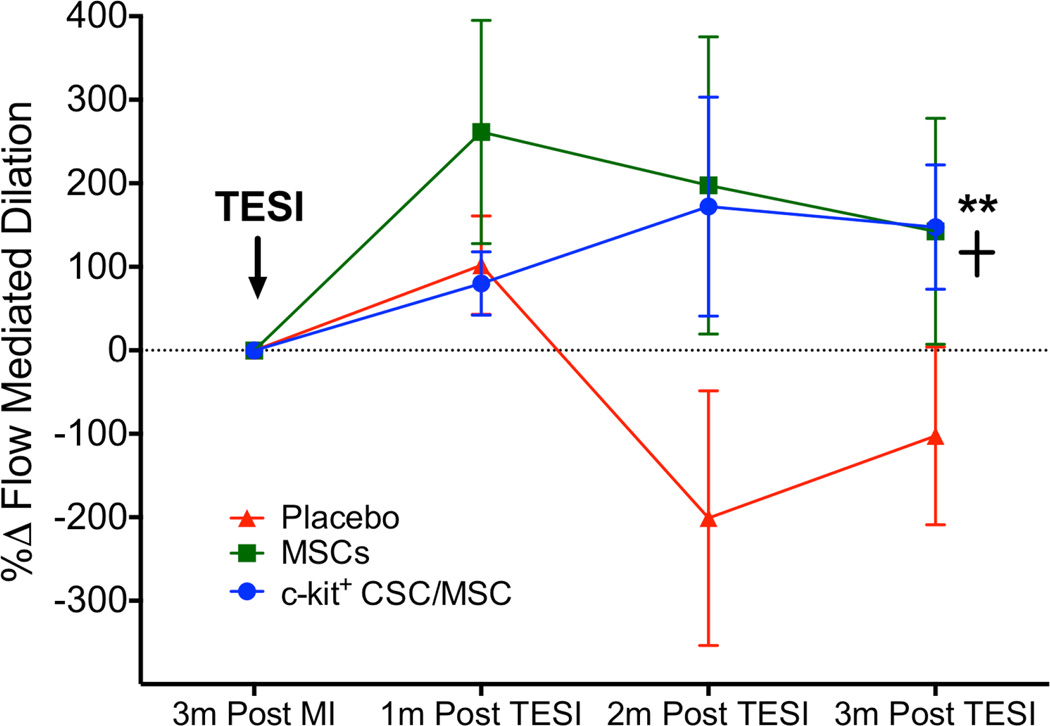
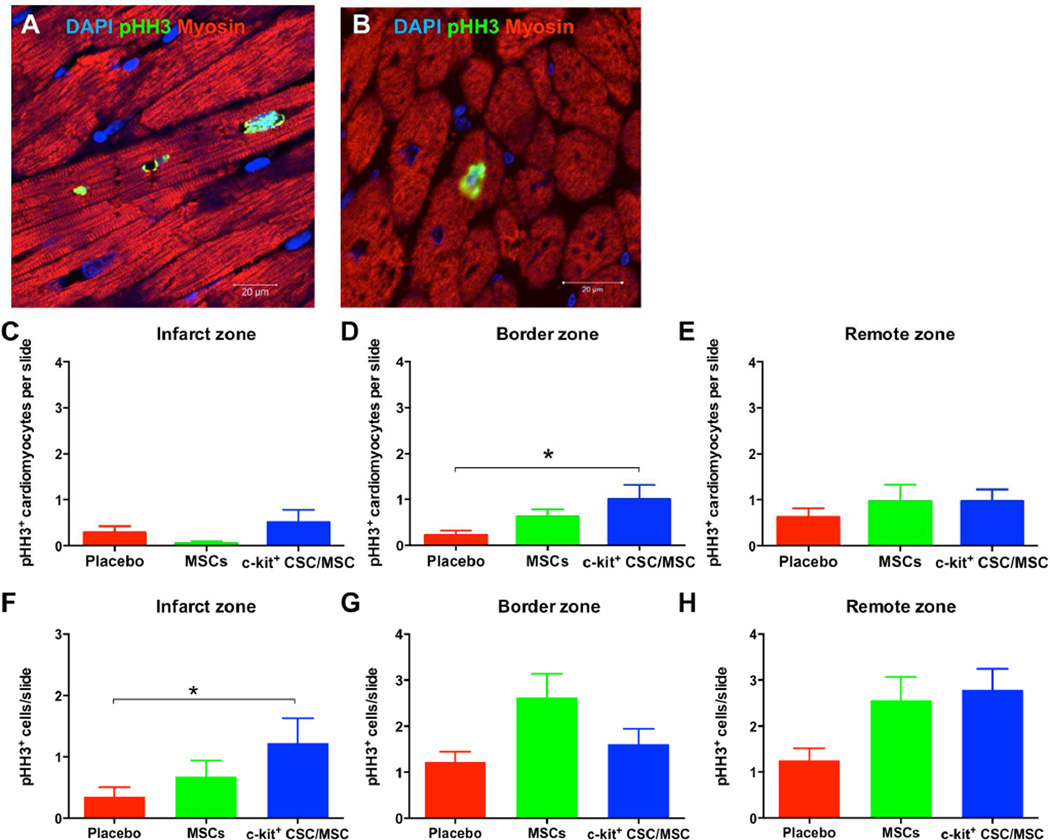
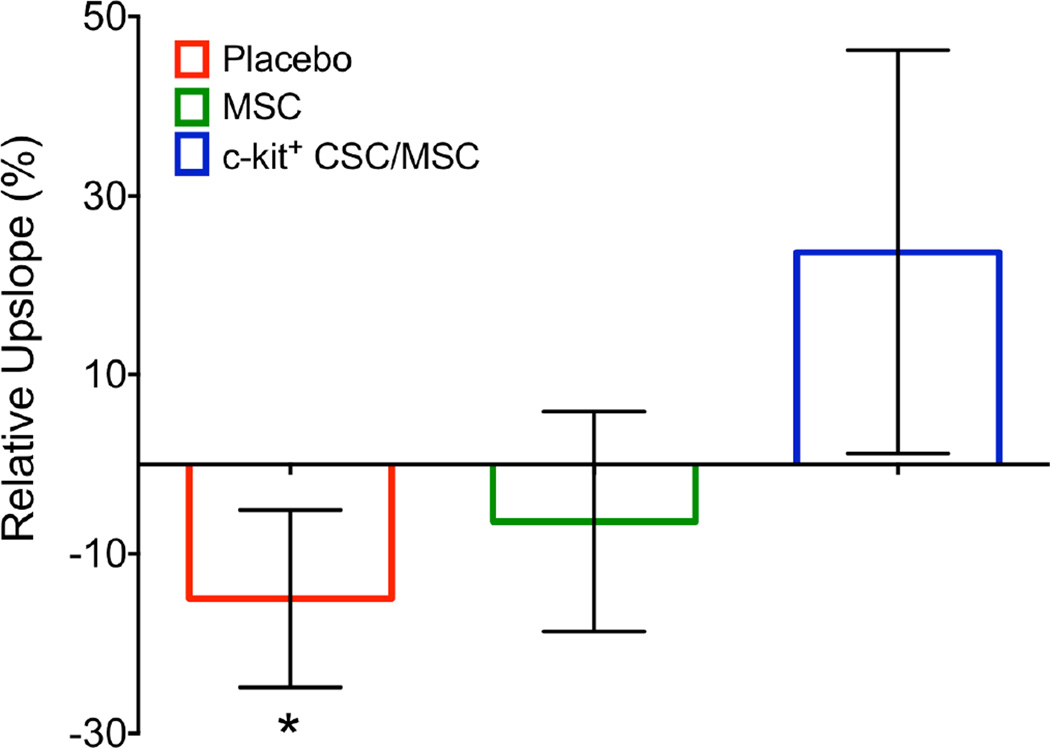
Results: Both groups of cell-treated animals exhibited significantly reduced scar size (MSCs -44.1 ± 6.8%; CSC/MSC -37.2 ± 5.4%; placebo -12.9 ± 4.2%; p < 0.0001), increased viable tissue, and improved wall motion relative to placebo 3 months post-injection. Ejection fraction (EF) improved (MSCs 2.9 ± 1.6 EF units; CSC/MSC 6.9 ± 2.8 EF units; placebo 2.5 ± 1.6 EF units; p = 0.0009), as did stroke volume, cardiac output, and diastolic strain only in the combination-treated animals, which also exhibited increased cardiomyocyte mitotic activity.
Conclusions: These findings illustrate that interactions between MSCs and CSCs enhance cardiac performance more than MSCs alone, establish the safety of autologous cell combination strategies, and support the development of second-generation cell therapeutic products.
Keywords: cardiac; combination therapy; heart failure; mesenchymal stem cell.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The other authors report no conflicts
Figures
Comment in
-
Cell Therapy Needs Rigorous Translational Studies in Large Animal Models.J Am Coll Cardiol. 2015 Nov 3;66(18):2000-2004. doi: 10.1016/j.jacc.2015.09.002. J Am Coll Cardiol. 2015. PMID: 26516003 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
