

Improved outcome with repeated intracoronary injection of bone marrow-derived cells within a registry: rationale for the randomized outcome trial REPEAT
- PMID: 26516172
- PMCID: PMC5841212
- DOI: 10.1093/eurheartj/ehv559
Improved outcome with repeated intracoronary injection of bone marrow-derived cells within a registry: rationale for the randomized outcome trial REPEAT
Abstract
Aims: Regenerative therapies have evolved as a promising new option in the treatment of post-infarction heart failure. A major limitation of intracoronary application of autologous bone marrow-derived mononuclear cells (BM-MNCs) is that homing of the applied cells is profoundly reduced in patients with post-infarction heart failure compared with patients with acute myocardial infarction. However, early pilot and also randomized controlled trials have demonstrated significant improvements in overall cardiac function. The aim of the present analysis was to quantify a potential mortality risk reduction and reduced hospitalization in order to provide data for a prospective outcome trial.
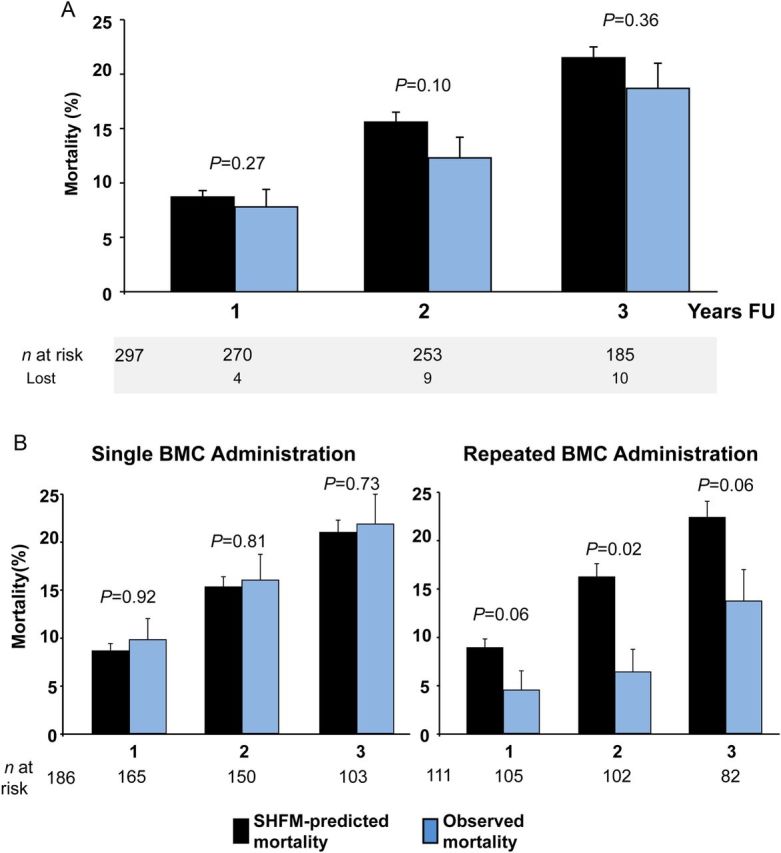
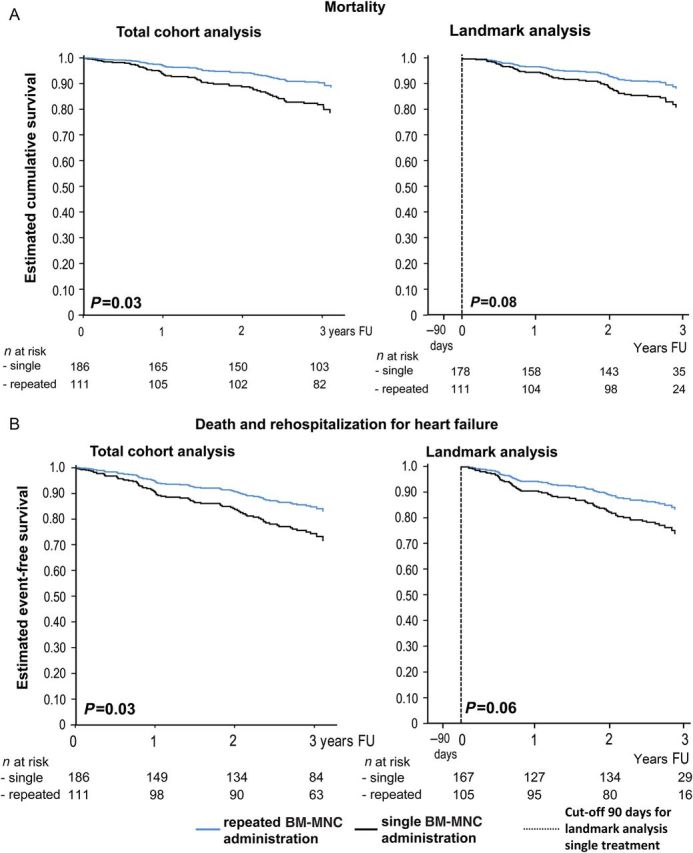
Methods and results: The results of an ongoing single-centre registry including 297 post-infarction heart failure patients suggest that repeated intracoronary application of autologous bone marrow-derived cells is associated with a significant better 2-year survival compared with a single BM-MNC application (2-year survival 93.6 vs. 84.0%, P = 0.03). Likewise, mortality is significantly lower at 2-year follow-up compared with the mortality estimated by the use of the Seattle Heart Failure Model (SHFM) in patients receiving repeated BM-MNC application (observed mortality 6.4%, predicted mortality 16.2%, P = 0.02). Although the trend persisted at 3-year follow-up, the mortality reduction was no longer statistically significant between single and repeated treatment (mortality 21.9 vs. 13.7%, P = 0.06).
Conclusion: Repeated intracoronary administration of BM-MNC appears to be associated with improved clinical outcome compared with single treatment at 2 years. This registry provides the rationale for the design of the multicentre randomized, controlled, open-label REPEAT trial, which prospectively compares the effects of single vs. repeated intracoronary application of autologous BM-MNC on total and SHFM-predicted mortality in patients with chronic post-infarction heart failure.
Keywords: Cell therapy; Chronic heart failure; Ischaemic cardiomyopathy; Outcome trial.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2015. For permissions please email: journals.permissions@oup.com.
Figures
Comment in
-
Repetition rescues regenerative reserve.Eur Heart J. 2016 Jun 1;37(21):1667-70. doi: 10.1093/eurheartj/ehv596. Epub 2015 Dec 5. Eur Heart J. 2016. PMID: 26637833 No abstract available.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB. Heart disease and stroke statistics-2015 update: a report from the American heart association. Circulation 2015;131:e29–e322. - PubMed
-
- Shafazand M, Schaufelberger M, Lappas G, Swedberg K, Rosengren A. Survival trends in men and women with heart failure of ischaemic and non-ischaemic origin: data for the period 1987-2003 from the Swedish Hospital Discharge Registry. Eur Heart J 2009;30:671–678. - PubMed
-
- Forbes SJ, Rosenthal N. Preparing the ground for tissue regeneration: from mechanism to therapy. Nat Med 2014;20:857–869. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
