

Cardiovascular disease in human immunodeficiency virus infected patients: A true or perceived risk?
- PMID: 26516417
- PMCID: PMC4620074
- DOI: 10.4330/wjc.v7.i10.633
Cardiovascular disease in human immunodeficiency virus infected patients: A true or perceived risk?
Abstract
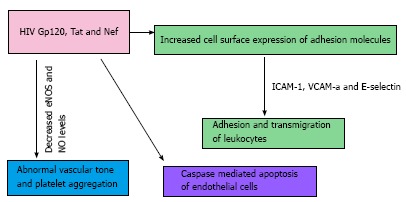
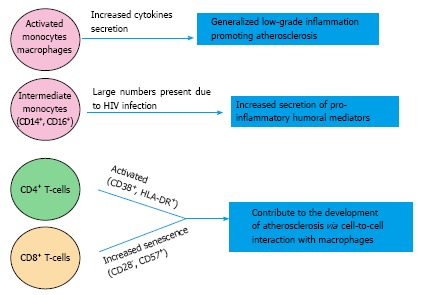
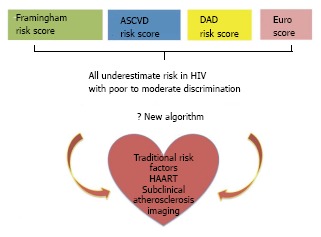
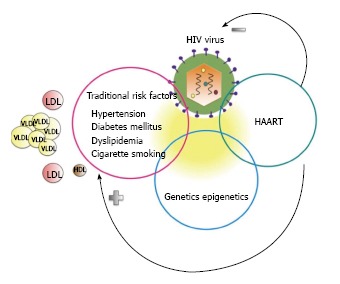
After the successful introduction of highly active antiretroviral agents the survival of patients infected with the human immunodeficiency virus (HIV) in developed countries has increased substantially. This has allowed the surfacing of several chronic diseases among which cardiovascular disease (CVD) is prominent. The pathogenesis of CVD in HIV is complex and involves a combination of traditional and HIV related factors. An accurate assessment of risk of CVD in these patients is still elusive and as a consequence the most appropriate preventive and therapeutic interventions remain controversial.
Keywords: Antiretroviral therapy; Atherosclerosis; Cardiovascular death; Cardiovascular risk; Dyslipidemia; Human immunodeficiency virus infection; Hypertension; Smoking.
Figures
References
-
- May MT, Sterne JA, Costagliola D, Sabin CA, Phillips AN, Justice AC, Dabis F, Gill J, Lundgren J, Hogg RS, et al. HIV treatment response and prognosis in Europe and North America in the first decade of highly active antiretroviral therapy: a collaborative analysis. Lancet. 2006;368:451–458. - PubMed
-
- Wada N, Jacobson LP, Cohen M, French A, Phair J, Muñoz A. Cause-specific life expectancies after 35 years of age for human immunodeficiency syndrome-infected and human immunodeficiency syndrome-negative individuals followed simultaneously in long-term cohort studies, 1984-2008. Am J Epidemiol. 2013;177:116–125. - PMC - PubMed
-
- van Sighem AI, Gras LA, Reiss P, Brinkman K, de Wolf F. Life expectancy of recently diagnosed asymptomatic HIV-infected patients approaches that of uninfected individuals. AIDS. 2010;24:1527–1535. - PubMed
-
- Schwarcz SK, Vu A, Hsu LC, Hessol NA. Changes in causes of death among persons with AIDS: San Francisco, California, 1996-2011. AIDS Patient Care STDS. 2014;28:517–523. - PubMed
-
- Mocroft A, Reiss P, Gasiorowski J, Ledergerber B, Kowalska J, Chiesi A, Gatell J, Rakhmanova A, Johnson M, Kirk O, et al. Serious fatal and nonfatal non-AIDS-defining illnesses in Europe. J Acquir Immune Defic Syndr. 2010;55:262–270. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
