

Epidural analgesia provides effective pain relief in patients undergoing open liver surgery
- PMID: 26516562
- PMCID: PMC4616967
- DOI: 10.1177/2049463714525140
Epidural analgesia provides effective pain relief in patients undergoing open liver surgery
Abstract
Background: Epidural analgesia has been the reference standard for the provision of post-operative pain relief in patients recovering from major upper abdominal operations, including liver resections. However, a failure rate of 20-32% has been reported.
Aim: The aim of the study was to analyse the success rates of epidural analgesia and the outcome in patients who underwent liver surgery.
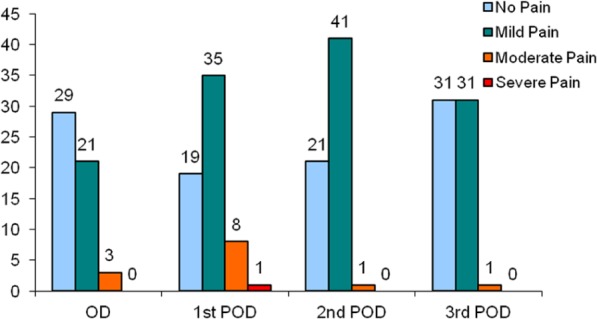
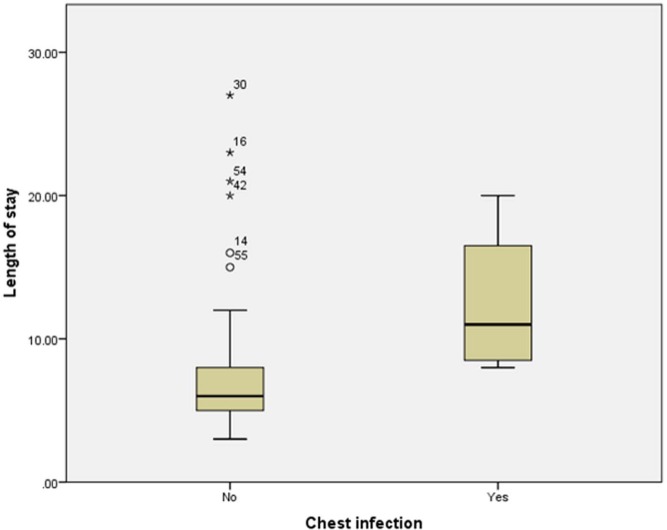
Methods: We collected data from a prospectively maintained database of 70 patients who underwent open liver surgery by a bilateral subcostal incision during a period of 20 months (February 2009 to September 2010). Anaesthetic consultants with expertise in anaesthesia for liver surgery performed the epidural catheter placement. A dedicated pain team assessed the post-operative pain scores on moving or coughing using the Verbal Descriptor Scale. The outcome was measured in terms of epidural success rates, pain scores, post-operative chest infection and length of hospital stay.
Results: The study group included 43 males and 27 females. The indication for resection was liver secondaries (70%), primary tumours (19%) and benign disease (11%). While major (≥3 segments) and minor resections (≤ 2 segments) were performed in 44% and 47% respectively, 9% of patients were inoperable. Epidural analgesia was successful in 64 patients (91%). Bacterial colonisation of epidural tip was noticed in two patients. However, no neurological complications were encountered. Five patients (7%) had radiologically confirmed chest infection. Four patients (6%) developed wound infection. One patient died due to liver failure following extended right hepatectomy and cholecystectomy for gall bladder cancer. The median length of stay was 6 days (3-27 days). The extent of liver resection (p = 0.026) and post-operative chest infection (p = 0.012) had a significant influence on the length of stay.
Conclusion: Our experience shows that epidural analgesia is safe and effective in providing adequate pain relief following open liver surgery.
Keywords: Epidural analgesia; acute pain; drug therapy; liver surgery; prevention and control.
Conflict of interest statement
Figures

References
-
- Werawatganon T, Charuluxanun S. Patient controlled intravenous opioid analgesia versus continuous epidural analgesia for pain after intra-abdominal surgery. Cochrane Database Syst Rev 2005; 1: CD004088. - PubMed
-
- Nishimori M, Ballantyne JC, Low JH. Epidural pain relief versus systemic opioid-based pain relief for abdominal aortic surgery. Cochrane Database Syst Rev 2006; 3: CD005059. - PubMed
-
- Kehlet H. Modification of responses to surgery by neural blockade: clinical implications. In: Cousins M, Bridenbaugh P. (eds) Neural blockade in clinical anesthesia and management of pain, 2nd edn. Philadelphia, PA: J. B. Lippincott & Co, 1988, pp. 145–188.
-
- Kehlet H, Holte K. Effect of postoperative analgesia on surgical outcome. Br J Anaesth 2001; 87(1): 62–72. - PubMed
-
- McLeod G, Davies H, Munnoch N, et al. Postoperative pain relief using thoracic epidural analgesia: outstanding success and disappointing failures. Anaesthesia 2001; 56(1): 75–81. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources