

Antibodies to MOG in adults with inflammatory demyelinating disease of the CNS
- PMID: 26516628
- PMCID: PMC4608758
- DOI: 10.1212/NXI.0000000000000163
Antibodies to MOG in adults with inflammatory demyelinating disease of the CNS
Abstract
Objective: To evaluate the clinical relevance of myelin oligodendrocyte glycoprotein antibody (MOG-Ab) in a cohort of adults with inflammatory demyelinating disease (IDD) of the CNS.
Methods: Live cell-based assays for MOG-Ab (IgG1 subset) and antibody to aquaporin-4 (AQP4-Ab) were performed in a cohort of 270 adult patients with IDD and 72 controls. Patients were first grouped by positive antibody result as MOG-Ab or AQP4-Ab, and the remainder were grouped by published diagnostic criteria.
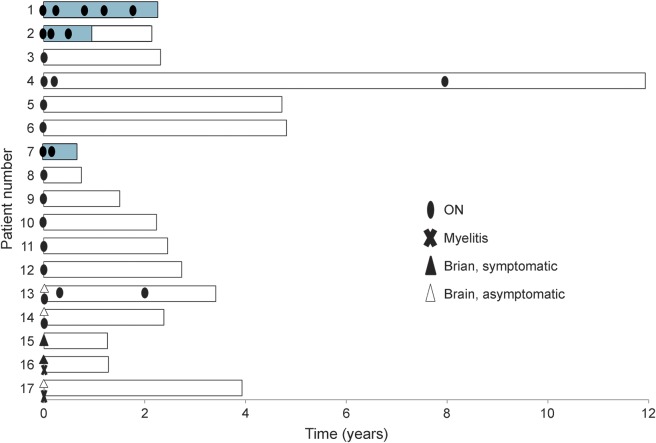
Results: Seventeen patients with IDD (6.3%) had MOG-Abs and 49 patients (18.1%) had AQP4-Abs; none had both antibodies. The MOG-Ab patients predominantly manifested with isolated symptoms of optic neuritis (83%). One-third of these patients experienced relapses, which involved only the optic nerve, and all relapsed within 1 year of disease onset. At onset, MRI in the MOG-Ab group uniquely demonstrated perineural enhancement, extending to the soft tissues around the optic nerves (33%). Although about 30% of MOG-Ab patients had brain MRI lesions, they had fewer periventricular lesions than the 26 patients with relapsing-remitting multiple sclerosis (MS); none of these lesions were ovoid or perpendicular to the ventricle. Moreover, MOG-Ab patients did not meet the diagnostic criteria for definite neuromyelitis optica (NMO) and had less spinal cord involvement than the AQP4-Ab group. Four patients (23.5%) had poor visual outcomes (<0.2) or paraplegia.
Conclusions: MOG-Abs may be a disease-specific biomarker in adult patients with IDD who have a disease distinct from NMO or MS. The radiologic as well as clinical manifestations of MOG-Ab patients can be useful in their differential diagnosis.
Figures



References
-
- Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006;66:1485–1489. - PubMed
-
- de Seze J, Debouverie M, Zephir H, et al. Acute fulminant demyelinating disease: a descriptive study of 60 patients. Arch Neurol 2007;64:1426–1432. - PubMed
-
- Shams P, Plant G. Optic neuritis: a review. Int MS J 2009;16:82–89. - PubMed
-
- Transverse Myelitis Consortium Working Group. Proposed diagnostic criteria and nosology of acute transverse myelitis. Neurology 2002;59:499–505. - PubMed
LinkOut - more resources
Full Text Sources