

Shared Decision Making and the Use of Decision Aids
- PMID: 26517595
- PMCID: PMC4640071
- DOI: 10.3238/arztebl.2015.0672
Shared Decision Making and the Use of Decision Aids
Abstract
Background: In shared decision making (SDM), the patient and the physician reach decisions in partnership. We conducted a trial of SDM training for physicians who treat patients with cancer.
Methods: Physicians who treat patients with cancer were invited to participate in a cluster-randomized trial and carry out SDM together with breast or colon cancer patients who faced decisions about their treatment. Decision-related physician-patient conversations were recorded. The patients filled out questionnaires immediately after the consultations (T1) and three months later (T2). The primary endpoints were the patients' confidence in and satisfaction with the decisions taken. The secondary endpoints were the process of decision making, anxiety, depression, quality of life, and externally assessed physician competence in SDM. The physicians in the intervention group underwent 12 hours of training in SDM, including the use of decision aids.
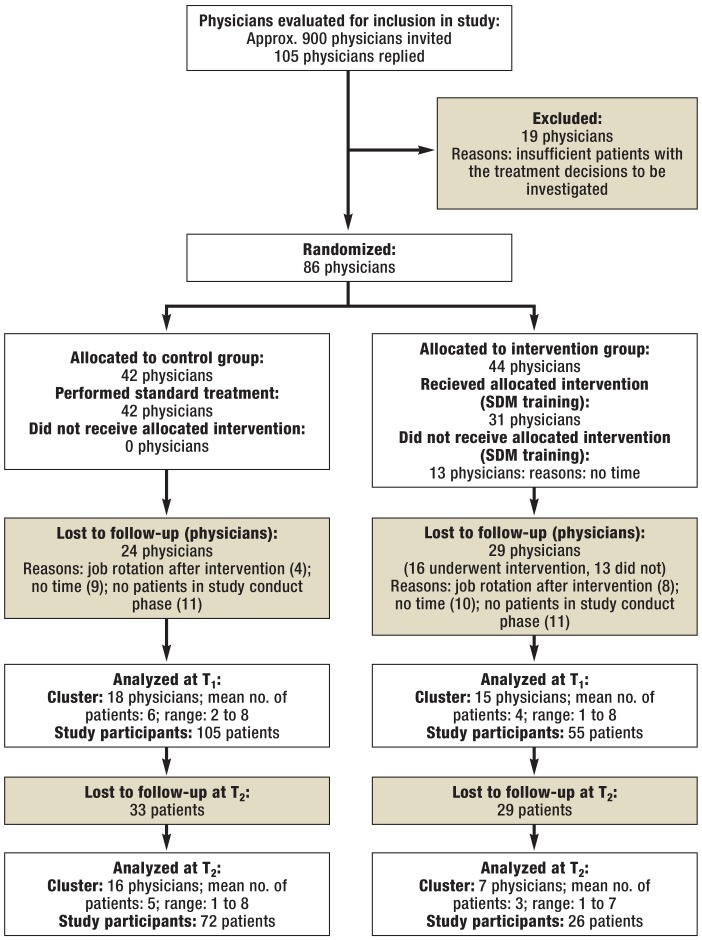
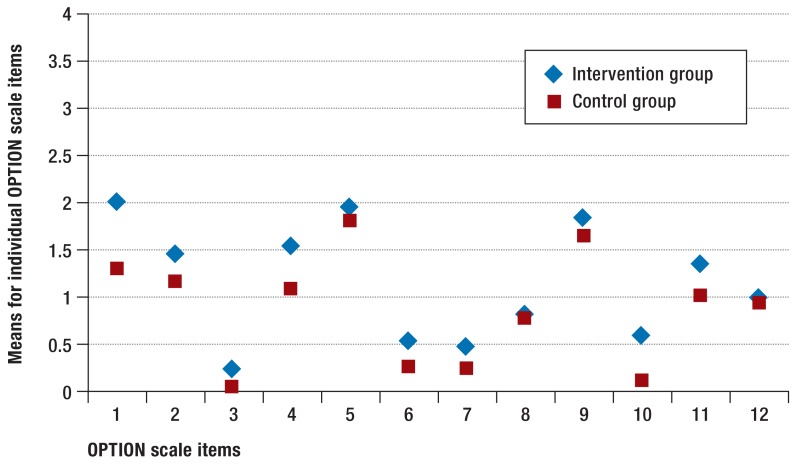
Results: Of the 900 physicians invited to participated in the trial, 105 answered the invitation. 86 were randomly assigned to either the intervention group or the control group (44 and 42 physicians, respectively); 33 of the 86 physicians recruited at least one patient for the trial. A total of 160 patients participated in the trial, of whom 55 were treated by physicians in the intervention group. There were no intergroup differences in the primary endpoints. Trained physicians were more competent in SDM (Cohen's d = 0.56; p<0.05). Patients treated by trained physicians had lower anxiety and depression scores immediately after the consultation (d = -0.12 and -0.14, respectively; p<0.10), and markedly lower anxiety and depression scores three months later (d = -0.94 and -0.67, p<0.01).
Conclusion: When physicians treating cancer patients improve their competence in SDM by appropriate training, their patients may suffer less anxiety and depression. These effects merit further study.
Figures
References
-
- Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Educ Couns. 2006;60:301–312. - PubMed
-
- Stacey D, Bennett CL, Barry MJ, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2011;10 CD001431. - PubMed
-
- Waljee JF, Rogers MAM, Alderman AK. Decision aids and breast cancer: do they influence choice for surgery and knowledge of treatment options? J Clin Oncol. 2007;25:1067–1073. - PubMed
-
- Whelan T, Levine M, Willan A, et al. Effect of a decision aid knowledge and treatment decision making for breast cancer surgery. A randomized trial. JAMA. 2004;292:435–441. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources