

Chronic traumatic encephalopathy pathology in a neurodegenerative disorders brain bank
- PMID: 26518018
- PMCID: PMC4655127
- DOI: 10.1007/s00401-015-1502-4
Chronic traumatic encephalopathy pathology in a neurodegenerative disorders brain bank
Abstract
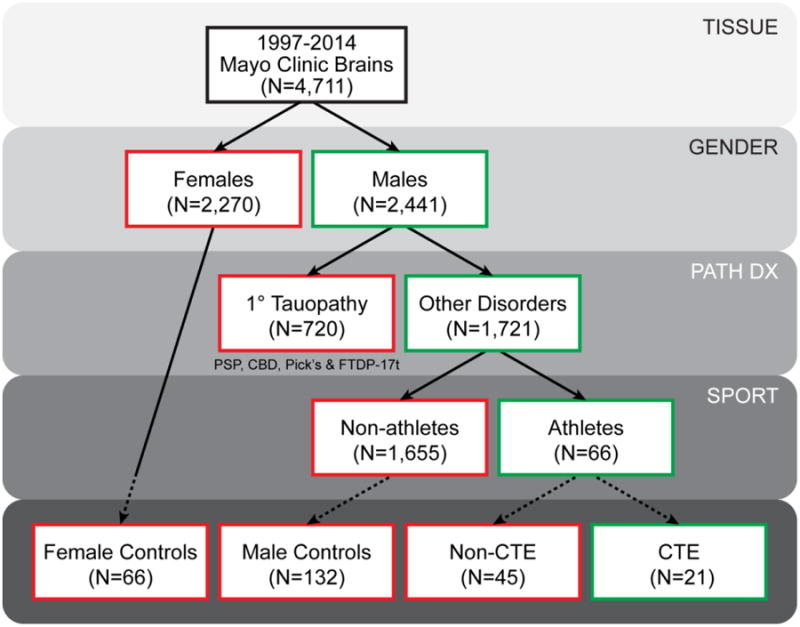
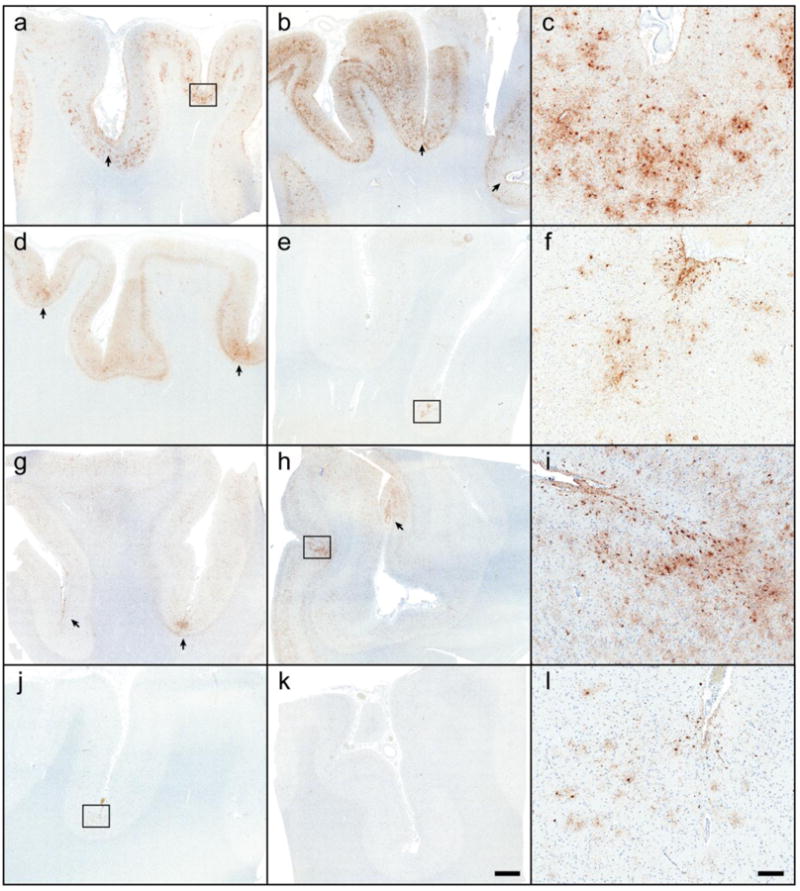
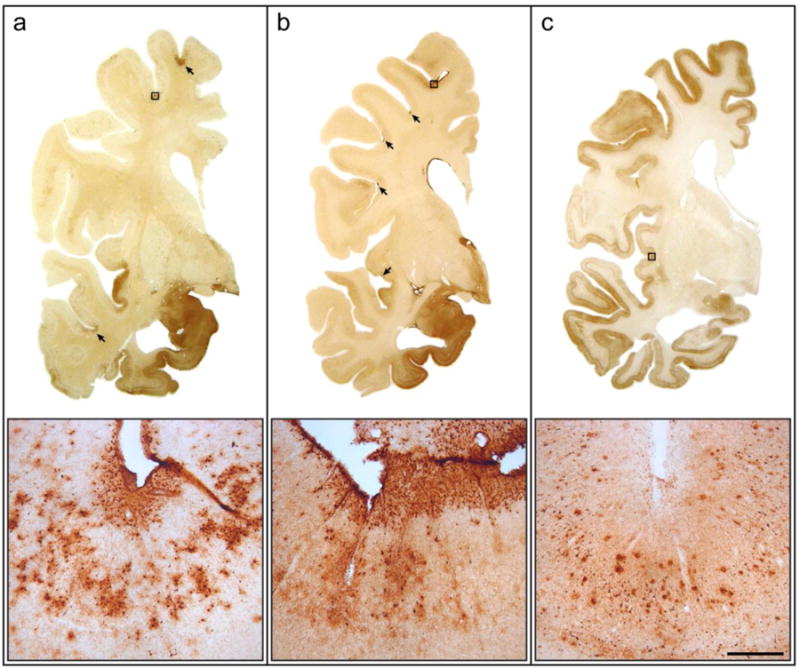
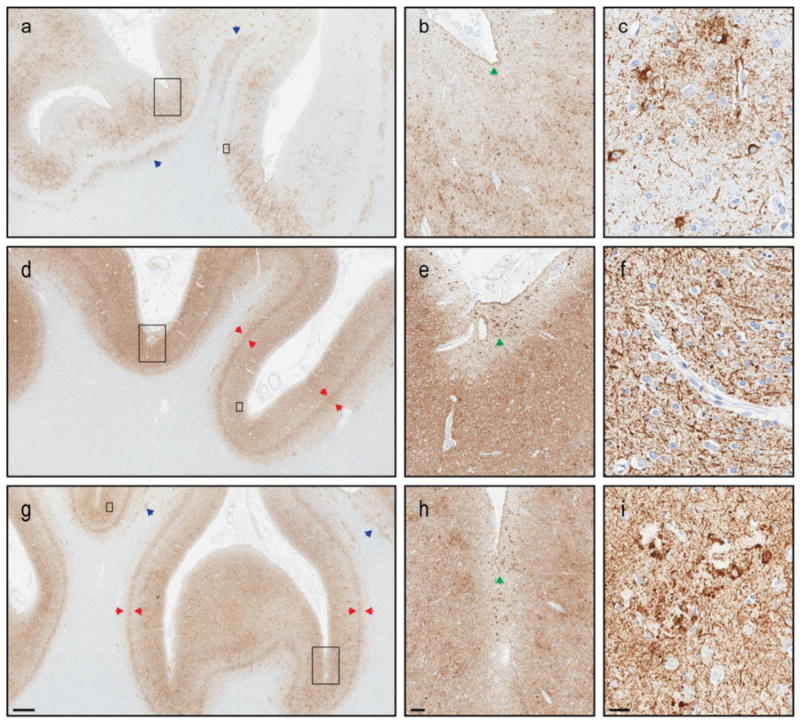
Chronic traumatic encephalopathy (CTE) is a progressive neurodegenerative disorder linked to repetitive traumatic brain injury (TBI) and characterized by deposition of hyperphosphorylated tau at the depths of sulci. We sought to determine the presence of CTE pathology in a brain bank for neurodegenerative disorders for individuals with and without a history of contact sports participation. Available medical records of 1721 men were reviewed for evidence of past history of injury or participation in contact sports. Subsequently, cerebral cortical samples were processed for tau immunohistochemistry in cases with a documented history of sports exposure as well as age- and disease-matched men and women without such exposure. For cases with available frozen tissue, genetic analysis was performed for variants in APOE, MAPT, and TMEM106B. Immunohistochemistry revealed 21 of 66 former athletes had cortical tau pathology consistent with CTE. CTE pathology was not detected in 198 individuals without exposure to contact sports, including 33 individuals with documented single-incident TBI sustained from falls, motor vehicle accidents, domestic violence, or assaults. Among those exposed to contact sports, those with CTE pathology did not differ from those without CTE pathology with respect to noted clinicopathologic features. There were no significant differences in genetic variants for those with CTE pathology, but we observed a slight increase in MAPT H1 haplotype, and there tended to be fewer homozygous carriers of the protective TMEM106B rs3173615 minor allele in those with sports exposure and CTE pathology compared to those without CTE pathology. In conclusion, this study has identified a small, yet significant, subset of individuals with neurodegenerative disorders and concomitant CTE pathology. CTE pathology was only detected in individuals with documented participation in contact sports. Exposure to contact sports was the greatest risk factor for CTE pathology. Future studies addressing clinical correlates of CTE pathology are needed.
Keywords: Brain bank; Chronic traumatic encephalopathy; Microtubule-associated protein tau; Sports; Traumatic brain injury.
Figures
References
-
- Braak H, Braak E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathologica. 1991;82:239–259. - PubMed
-
- Cantu RC, Mueller FO. The prevention of catastrophic head and spine injuries in high school and college sports. Br J Sports Med. 2009;43:981–986. - PubMed
-
- Corsellis JA, Bruton CJ, Freeman-Browne D. The aftermath of boxing. Psychological Medicine. 1973;3:270–303. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
