

Complement inhibitors to treat IgM-mediated autoimmune hemolysis
- PMID: 26521297
- PMCID: PMC4825292
- DOI: 10.3324/haematol.2015.128538
Complement inhibitors to treat IgM-mediated autoimmune hemolysis
Abstract
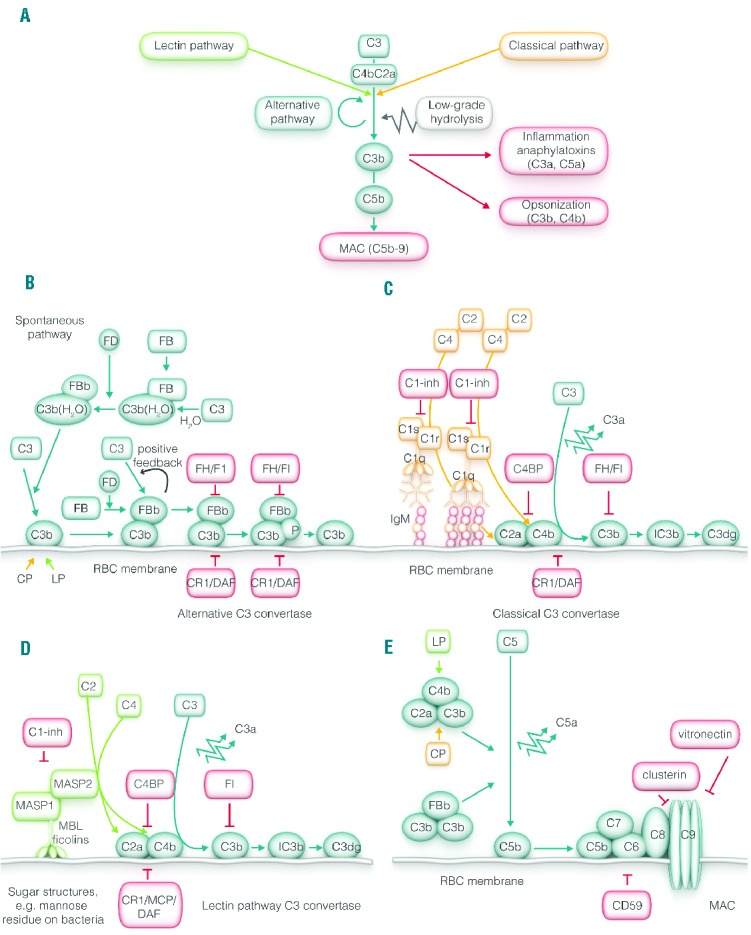
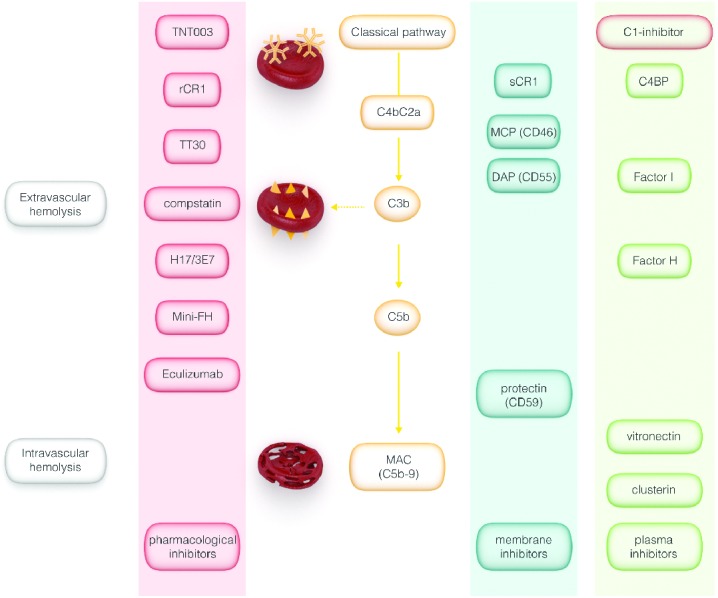
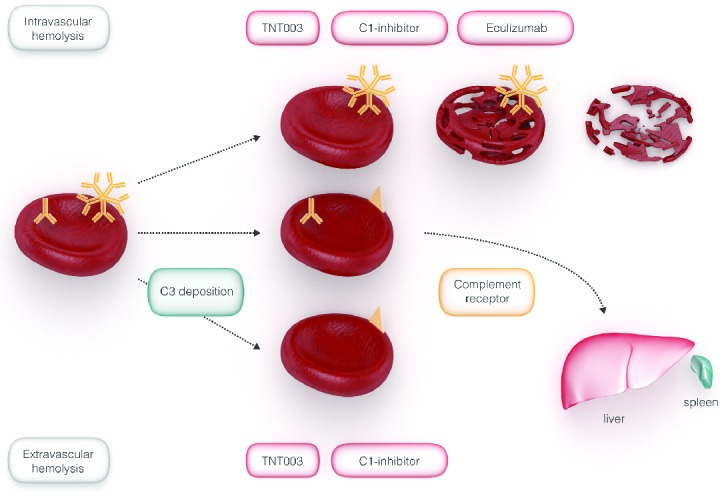
Complement activation in autoimmune hemolytic anemia may exacerbate extravascular hemolysis and may occasionally result in intravascular hemolysis. IgM autoantibodies as characteristically found in cold autoantibody autoimmune hemolytic anemia, in cold agglutinin disease but also in a considerable percentage of patients with warm autoantibodies are very likely to activate complement in vivo. Therapy of IgM-mediated autoimmune hemolytic anemia mainly aims to decrease autoantibody production. However, most of these treatments require time to become effective and will not stop immediate ongoing complement-mediated hemolysis nor prevent hemolysis of transfused red blood cells. Therefore pharmacological inhibition of the complement system might be a suitable approach to halt or at least attenuate ongoing hemolysis and improve the recovery of red blood cell transfusion in autoimmune hemolytic anemia. In recent years, several complement inhibitors have become available in the clinic, some of them with proven efficacy in autoimmune hemolytic anemia. In the present review, we give a short introduction on the pathogenesis of autoimmune hemolytic anemia, followed by an overview on the complement system with a special focus on its regulation. Finally, we will discuss complement inhibitors with regard to their potential efficacy to halt or attenuate hemolysis in complement-mediated autoimmune hemolytic anemia.
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Packman CH. Hemolytic anemia due to warm autoantibodies. Blood Rev 2008;22 (1):17–31. - PubMed
-
- Petz LD. Cold antibody autoimmune hemolytic anemias. Blood Rev 2008; 22(1): 1–15. - PubMed
-
- Zeerleder S. Autoimmune haemolytic anaemia - a practical guide to cope with a diagnostic and therapeutic challenge. Neth J Med 2011;69(4):177–184. - PubMed
-
- Barcellini W, Fattizzo B, Zaninoni A, et al. Clinical heterogeneity and predictors of outcome in primary autoimmune hemolytic anemia: a GIMEMA study of 308 patients. Blood 2014;124(19):2930–2936. - PubMed
-
- Lechner K, Jager U. How I treat autoimmune hemolytic anemias in adults. Blood 2010;116(11):1831–1838. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
