

Hypofractionated radiotherapy versus conventionally fractionated radiotherapy for patients with intermediate-risk localised prostate cancer: 2-year patient-reported outcomes of the randomised, non-inferiority, phase 3 CHHiP trial
- PMID: 26522334
- PMCID: PMC4664817
- DOI: 10.1016/S1470-2045(15)00280-6
Hypofractionated radiotherapy versus conventionally fractionated radiotherapy for patients with intermediate-risk localised prostate cancer: 2-year patient-reported outcomes of the randomised, non-inferiority, phase 3 CHHiP trial
Abstract
Background: Patient-reported outcomes (PROs) might detect more toxic effects of radiotherapy than do clinician-reported outcomes. We did a quality of life (QoL) substudy to assess PROs up to 24 months after conventionally fractionated or hypofractionated radiotherapy in the Conventional or Hypofractionated High Dose Intensity Modulated Radiotherapy in Prostate Cancer (CHHiP) trial.
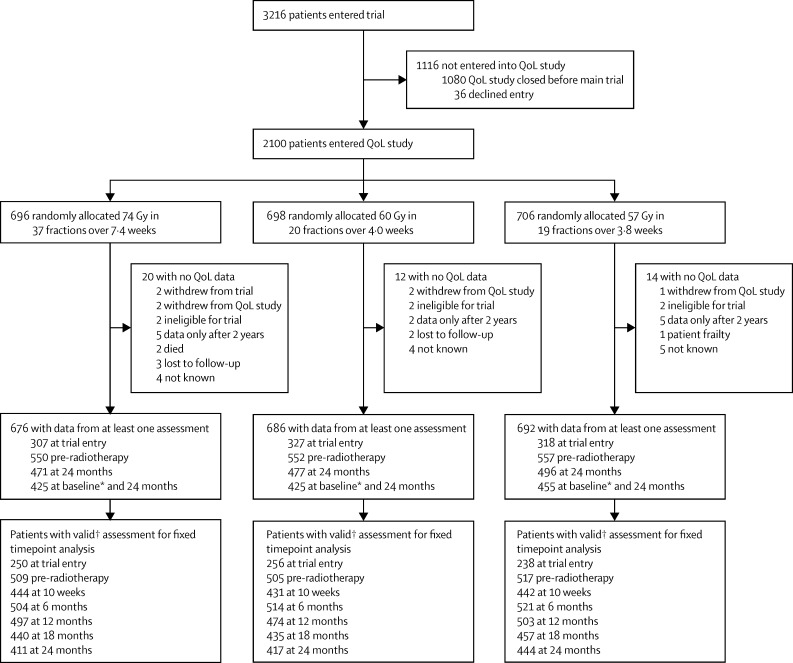
Methods: The CHHiP trial is a randomised, non-inferiority phase 3 trial done in 71 centres, of which 57 UK hospitals took part in the QoL substudy. Men with localised prostate cancer who were undergoing radiotherapy were eligible for trial entry if they had histologically confirmed T1b-T3aN0M0 prostate cancer, an estimated risk of seminal vesicle involvement less than 30%, prostate-specific antigen concentration less than 30 ng/mL, and a WHO performance status of 0 or 1. Participants were randomly assigned (1:1:1) to receive a standard fractionation schedule of 74 Gy in 37 fractions or one of two hypofractionated schedules: 60 Gy in 20 fractions or 57 Gy in 19 fractions. Randomisation was done with computer-generated permuted block sizes of six and nine, stratified by centre and National Comprehensive Cancer Network (NCCN) risk group. Treatment allocation was not masked. UCLA Prostate Cancer Index (UCLA-PCI), including Short Form (SF)-36 and Functional Assessment of Cancer Therapy-Prostate (FACT-P), or Expanded Prostate Cancer Index Composite (EPIC) and SF-12 quality-of-life questionnaires were completed at baseline, pre-radiotherapy, 10 weeks post-radiotherapy, and 6, 12, 18, and 24 months post-radiotherapy. The CHHiP trial completed accrual on June 16, 2011, and the QoL substudy was closed to further recruitment on Nov 1, 2009. Analysis was on an intention-to-treat basis. The primary endpoint of the QoL substudy was overall bowel bother and comparisons between fractionation groups were done at 24 months post-radiotherapy. The CHHiP trial is registered with ISRCTN registry, number ISRCTN97182923.
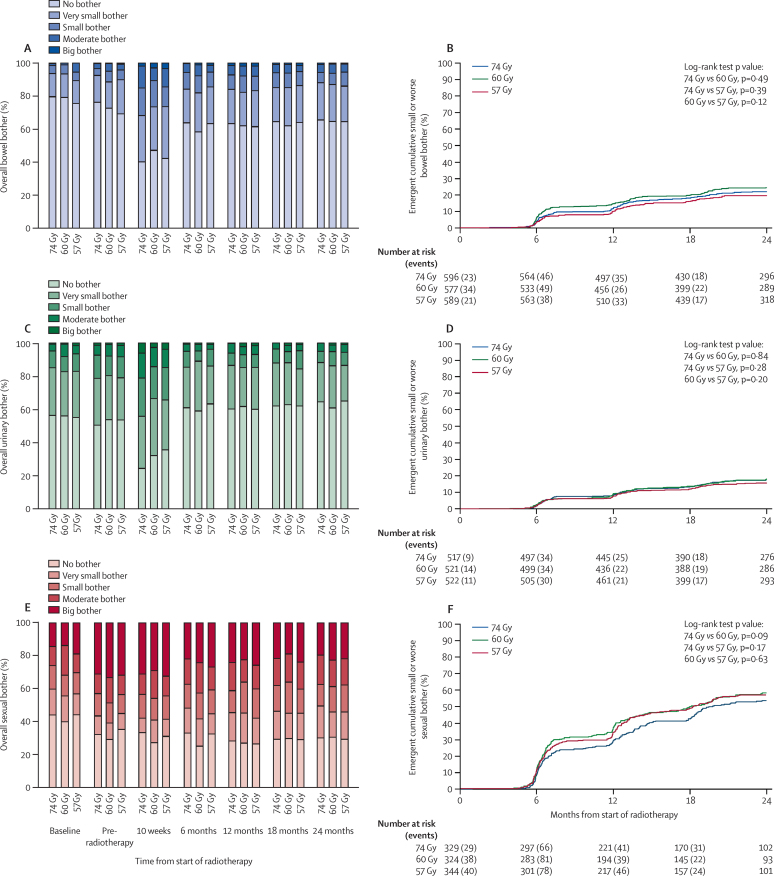
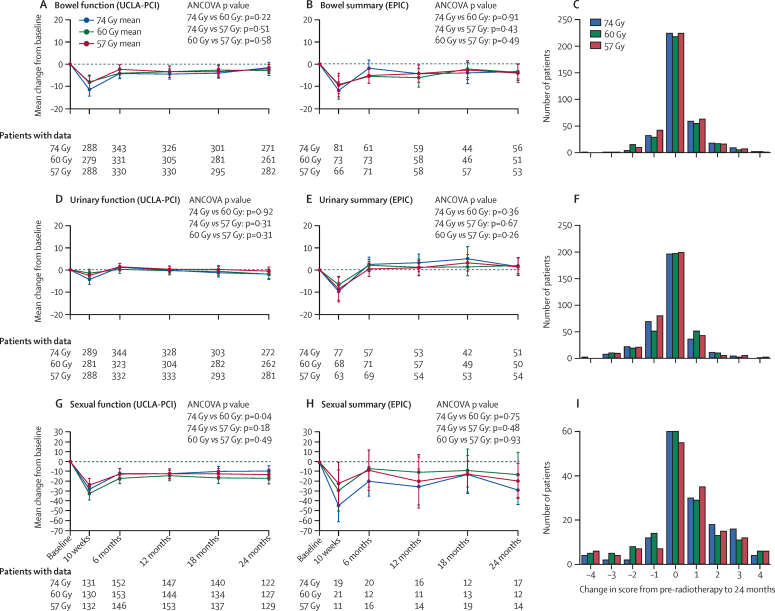
Findings: 2100 participants in the CHHiP trial consented to be included in the QoL substudy: 696 assigned to the 74 Gy schedule, 698 assigned to the 60 Gy schedule, and 706 assigned to the 57 Gy schedule. Of these individuals, 1659 (79%) provided data pre-radiotherapy and 1444 (69%) provided data at 24 months after radiotherapy. Median follow-up was 50·0 months (IQR 38·4-64·2) on April 9, 2014, which was the most recent follow-up measurement of all data collected before the QoL data were analysed in September, 2014. Comparison of 74 Gy in 37 fractions, 60 Gy in 20 fractions, and 57 Gy in 19 fractions groups at 2 years showed no overall bowel bother in 269 (66%), 266 (65%), and 282 (65%) men; very small bother in 92 (22%), 91 (22%), and 93 (21%) men; small bother in 26 (6%), 28 (7%), and 38 (9%) men; moderate bother in 19 (5%), 23 (6%), and 21 (5%) men, and severe bother in four (<1%), three (<1%) and three (<1%) men respectively (74 Gy vs 60 Gy, ptrend=0.64, 74 Gy vs 57 Gy, ptrend=0·59). We saw no differences between treatment groups in change of bowel bother score from baseline or pre-radiotherapy to 24 months.
Interpretation: The incidence of patient-reported bowel symptoms was low and similar between patients in the 74 Gy control group and the hypofractionated groups up to 24 months after radiotherapy. If efficacy outcomes from CHHiP show non-inferiority for hypofractionated treatments, these findings will add to the growing evidence for moderately hypofractionated radiotherapy schedules becoming the standard treatment for localised prostate cancer.
Funding: Cancer Research UK, Department of Health, and the National Institute for Health Research Cancer Research Network.
Copyright © 2015 Wilkins et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Hypofractionation for prostate cancer and PROs.Lancet Oncol. 2015 Dec;16(16):1570-1. doi: 10.1016/S1470-2045(15)00364-2. Epub 2015 Oct 28. Lancet Oncol. 2015. PMID: 26522335 No abstract available.
-
Re: Hypofractionated Radiotherapy versus Conventionally Fractionated Radiotherapy for Patients with Intermediate-Risk Localised Prostate Cancer: 2-Year Patient-Reported Outcomes of the Randomised, Non-Inferiority, Phase 3 CHHiP Trial.J Urol. 2016 Nov;196(5):1445-1447. doi: 10.1016/j.juro.2016.08.067. Epub 2016 Aug 23. J Urol. 2016. PMID: 27751451 No abstract available.
References
-
- Cancer Research UK. Prostate cancer statistics—key facts. http://info.cancerresearchuk.org/cancerstats/keyfacts/prostate-cancer/ (accessed June 6 2015).
-
- Sonn GA, Sadetsky N, Presti JC, Litwin MS. Differing perceptions of quality of life in patients with prostate cancer and their doctors. J Urol. 2013;189:S59–S65. - PubMed
-
- Litwin MS, Lubeck DP, Henning JM, Carroll PR. Differences in urologist and patient assessments of health related quality of life in men with prostate cancer: results of the CaPSURE database. J Urol. 1998;159:1988–1992. - PubMed
-
- Dearnaley D, Syndikus I, Sumo G. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: preliminary safety results from the CHHiP randomised controlled trial. Lancet Oncol. 2012;13:43–54. - PubMed
-
- Litwin MS, Hays RD, Fink A, Ganz PA, Leake B, Brook RH. The UCLA Prostate Cancer Index: development, reliability, and validity of a health-related quality of life measure. Med Care. 1998;36:1002–1012. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
