

Ventilator-Associated Events in Neonates and Children--A New Paradigm
- PMID: 26524075
- PMCID: PMC10884951
- DOI: 10.1097/CCM.0000000000001372
Ventilator-Associated Events in Neonates and Children--A New Paradigm
Abstract
Objectives: To identify a pediatric ventilator-associated condition definition for use in neonates and children by exploring whether potential ventilator-associated condition definitions identify patients with worse outcomes.
Design: Retrospective cohort study and a matched cohort analysis.
Setting: Pediatric, cardiac, and neonatal ICUs in five U.S. hospitals.
Patients: Children 18 years old or younger ventilated for at least 1 day.
Interventions: None.
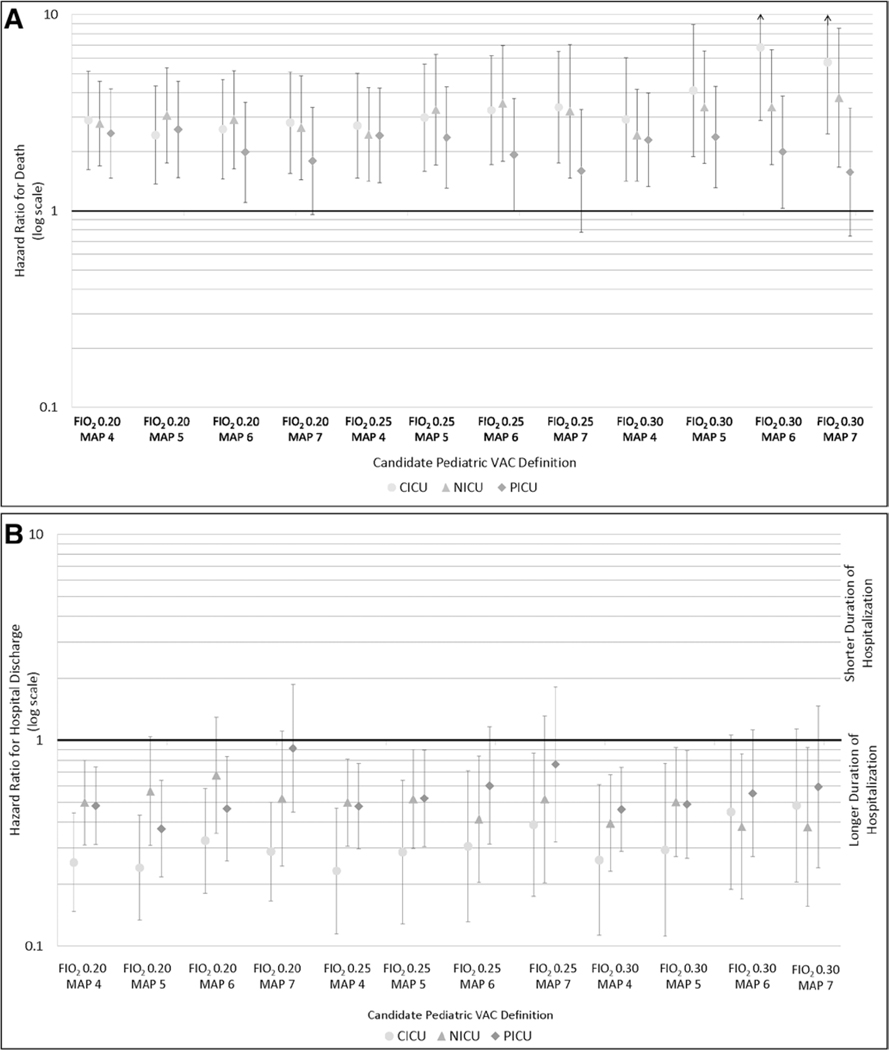
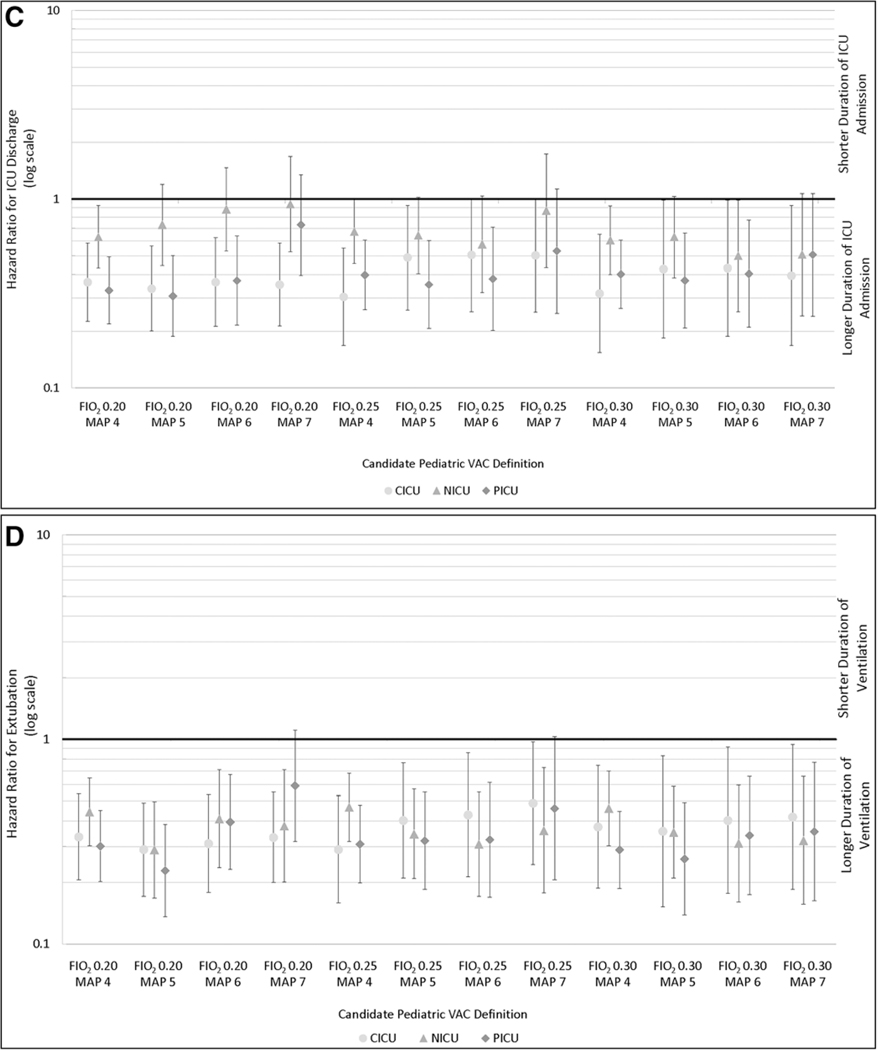
Measurements and main results: We evaluated the evidence of worsening oxygenation via a range of thresholds for increases in daily minimum fraction of inspired oxygen (by 0.20, 0.25, and 0.30) and daily minimum mean airway pressure (by 4, 5, 6, and 7 cm H2O). We required worsening oxygenation be sustained for at least 2 days after at least 2 days of stability. We matched patients with a ventilator-associated condition to those without and used Cox proportional hazard models with frailties to examine associations with hospital mortality, hospital and ICU length of stay, and duration of ventilation. The cohort included 8,862 children with 10,209 hospitalizations and 77,751 ventilator days. For the fraction of inspired oxygen 0.25/mean airway pressure 4 definition (i.e., increase in minimum daily fraction of inspired oxygen by 0.25 or mean airway pressure by 4), rates ranged from 2.9 to 3.2 per 1,000 ventilator days depending on ICU type; the fraction of inspired oxygen 0.30/mean airway pressure 7 definition yielded ventilator-associated condition rates of 1.1-1.3 per 1,000 ventilator days. All definitions were significantly associated with greater risk of hospital death, with hazard ratios ranging from 1.6 (95% CI, 0.7-3.4) to 6.8 (2.9-16.0), depending on thresholds and ICU type. Each definition was associated with prolonged hospitalization, time in ICU, and duration of ventilation, among survivors. The advisory board of the study proposed using the fraction of inspired oxygen 0.25/mean airway pressure 4 thresholds to identify pediatric ventilator-associated conditions in ICUs.
Conclusions: Pediatric patients with ventilator-associated conditions are at substantially higher risk for mortality and morbidity across ICUs, regardless of thresholds used. Next steps include identification of risk factors, etiologies, and preventative measures for pediatric ventilator-associated conditions.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest. The findings and conclusions in this report are those of the author(s) and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Figures

Comment in
-
Ventilator-Associated Events in Neonates and Children: A Single Definition for a Heterogeneous Population.Crit Care Med. 2016 Jan;44(1):233-4. doi: 10.1097/CCM.0000000000001443. Crit Care Med. 2016. PMID: 26672928 No abstract available.
References
-
- Centers for Disease Control and Prevention (CDC). Ventilator-Associated Event (VAE) Protocol, 2013. Atlanta, Centers for Disease Control and Prevention (CDC). Available at: http://www.cdc.gov/nhsn/acutecare-hospital/vae/. Accessed February 18, 2015
-
- National Conference of State Legislatures (NCSL): Medicare Nonpayment for Medical Errors. Washington, DC, National Conference of State Legislatures (NCSL), 2008. Available at: http://www.ncsl.org/Portals/1/documents/health/MCHAC.pdf. Accessed September 25, 2015
-
- Halpern NA, Hale KE, Sepkowitz KA, et al.: A world without ventilator-associated pneumonia: Time to abandon surveillance and deconstruct the bundle. Crit Care Med 2012; 40:267–270 - PubMed
-
- Agency for Healthcare Research and Quality (AHRQ). RACHS-1 Pediatric Heart Surgery Volume, Technical Specifications, Pediatric Quality Indicators #7 (PDI #7), Version 4.5. 2013. Available at: http://www.qualityindicators.ahrq.gov/Downloads/Modules/PDI/V45/TechSpec.... Accessed September 25, 2015
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
