

Circulating tumor DNA to monitor treatment response and detect acquired resistance in patients with metastatic melanoma
- PMID: 26524482
- PMCID: PMC4747205
- DOI: 10.18632/oncotarget.5788
Circulating tumor DNA to monitor treatment response and detect acquired resistance in patients with metastatic melanoma
Abstract
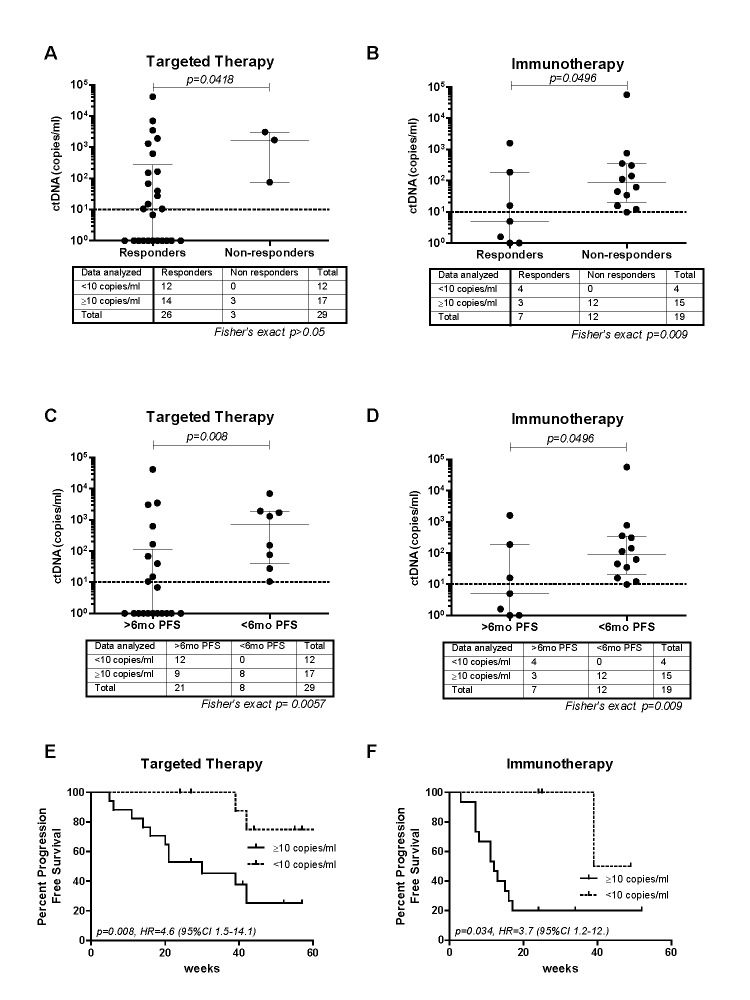
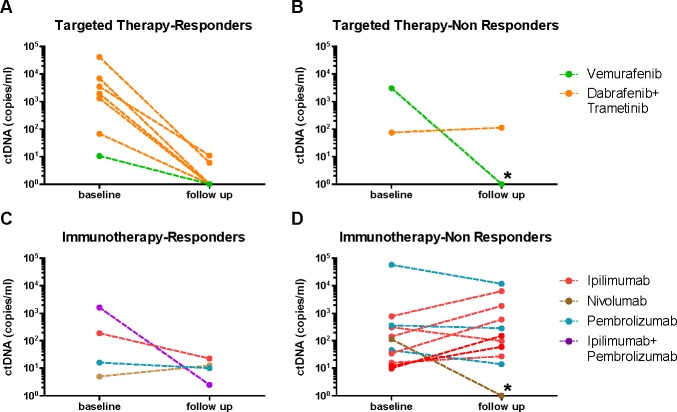
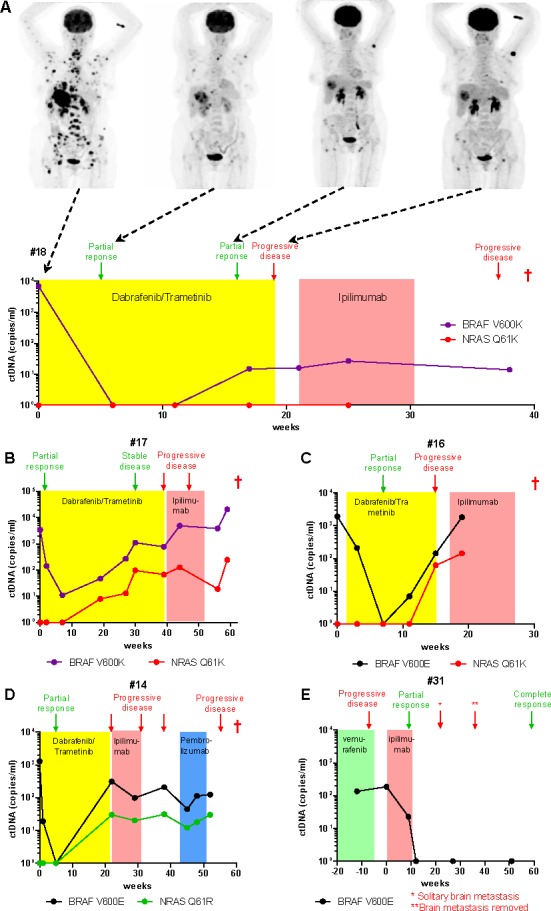
Repeat tumor biopsies to study genomic changes during therapy are difficult, invasive and data are confounded by tumoral heterogeneity. The analysis of circulating tumor DNA (ctDNA) can provide a non-invasive approach to assess prognosis and the genetic evolution of tumors in response to therapy. Mutation-specific droplet digital PCR was used to measure plasma concentrations of oncogenic BRAF and NRAS variants in 48 patients with advanced metastatic melanoma prior to treatment with targeted therapies (vemurafenib, dabrafenib or dabrafenib/trametinib combination) or immunotherapies (ipilimumab, nivolumab or pembrolizumab). Baseline ctDNA levels were evaluated relative to treatment response and progression-free survival (PFS). Tumor-associated ctDNA was detected in the plasma of 35/48 (73%) patients prior to treatment and lower ctDNA levels at this time point were significantly associated with response to treatment and prolonged PFS, irrespective of therapy type. Levels of ctDNA decreased significantly in patients treated with MAPK inhibitors (p < 0.001) in accordance with response to therapy, but this was not apparent in patients receiving immunotherapies. We show that circulating NRAS mutations, known to confer resistance to BRAF inhibitors, were detected in 3 of 7 (43%) patients progressing on kinase inhibitor therapy. Significantly, ctDNA rebound and circulating mutant NRAS preceded radiological detection of progressive disease. Our data demonstrate that ctDNA is a useful biomarker of response to kinase inhibitor therapy and can be used to monitor tumor evolution and detect the early appearance of resistance effectors.
Keywords: MAPK inhibition; acquired resistance; ctDNA; immunotherapy; melanoma.
Conflict of interest statement
G. Long has served as a consultant advisor for Amgen, BMS, GSK, Merck MSD, Novartis, and Roche. R.A. Scolyer has received speaker's bureau honoraria from Roche and is consultant/advisory board member for GlaxoSmithKline. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S, Teague J, Woffendin H, Garnett MJ, Bottomley W, Davis N, Dicks E, Ewing R, Floyd Y, Gray K, Hall S, et al. Mutations of the BRAF gene in human cancer. Nature. 2002;417:949–954. - PubMed
-
- Lovly CM, Dahlman KB, Fohn LE, Su Z, Dias-Santagata D, Hicks DJ, Hucks D, Berry E, Terry C, Duke M, Su Y, Sobolik-Delmaire T, Richmond A, Kelley MC, Vnencak-Jones CL, Iafrate AJ, et al. Routine multiplex mutational profiling of melanomas enables enrollment in genotype-driven therapeutic trials. PLoS One. 2012;7:e35309. - PMC - PubMed
-
- Klein O, Clements A, Menzies AM, O'Toole S, Kefford RF, Long GV. BRAF inhibitor activity in V600R metastatic melanoma. European journal of cancer. 2013;49:1073–1079. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
