

Association Between Anemia, Bleeding, and Transfusion with Long-term Mortality Following Noncardiac Surgery
- PMID: 26524702
- PMCID: PMC5567997
- DOI: 10.1016/j.amjmed.2015.10.012
Association Between Anemia, Bleeding, and Transfusion with Long-term Mortality Following Noncardiac Surgery
Abstract
Background: Preoperative anemia is a well-established risk factor for short-term mortality in patients undergoing noncardiac surgery, but appropriate thresholds for transfusion remain uncertain. The objective of this study was to determine long-term outcomes associated with anemia, hemorrhage, and red blood cell transfusion in patients undergoing noncardiac surgery.
Methods: We performed a long-term follow-up study of consecutive subjects undergoing hip, knee, and spine surgery between November 1, 2008 and December 31, 2009. Clinical data were obtained from administrative and laboratory databases, and retrospective record review. Preoperative anemia was defined as baseline hemoglobin < 13 g/dL for men and < 12 g/dL for women. Hemorrhage was defined by International Classification of Diseases, Ninth Revision coding. Data on long-term survival were collected from the Social Security Death Index database. Logistic regression models were used to identify factors associated with long-term mortality.
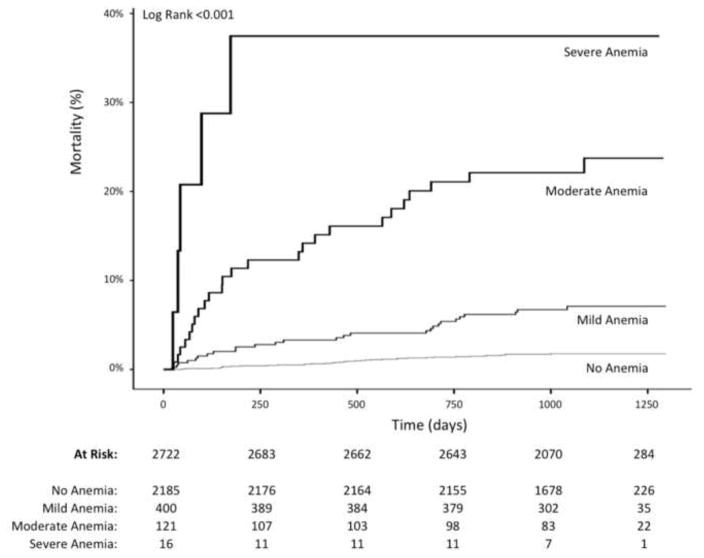
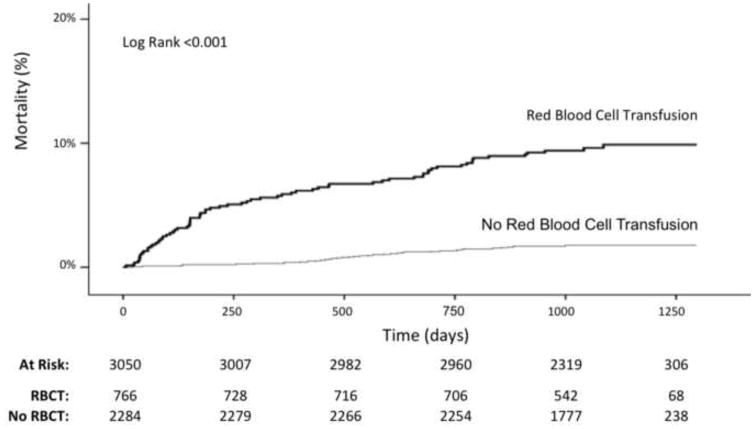
Results: There were 3050 subjects who underwent orthopedic surgery. Preoperative anemia was present in 17.6% (537) of subjects, hemorrhage occurred in 33 (1%), and 766 (25%) received at least one red blood cell transfusion. Over 9015 patient-years of follow-up, 111 deaths occurred. Anemia (hazard ratio [HR] 3.91; confidence interval [CI], 2.49-6.15) and hemorrhage (HR 5.28; 95% CI, 2.20-12.67) were independently associated with long-term mortality after multivariable adjustment. Red blood cell transfusion during the surgical hospitalization was associated with long-term mortality (HR 3.96; 95% CI, 2.47-6.34), which was attenuated by severity of anemia (no anemia [HR 4.39], mild anemia [HR 2.27], and moderate/severe anemia [HR 0.81]; P for trend .0015).
Conclusions: Preoperative anemia, perioperative bleeding, and red blood cell transfusion are associated with increased mortality at long-term follow-up after noncardiac surgery. Strategies to minimize anemia and bleeding should be considered for all patients, and restrictive transfusion strategies may be advisable. Further investigation into mechanisms of these adverse events is warranted.
Keywords: Anemia; Hemorrhage; Mortality; Red blood cells; Surgery; Transfusion.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest: None
Figures
Comment in
-
Assessing Association Among Anemia, Bleeding, and Transfusion with Long-Term Mortality.Am J Med. 2016 Sep;129(9):e209. doi: 10.1016/j.amjmed.2015.11.036. Am J Med. 2016. PMID: 27554962 No abstract available.
-
The Reply.Am J Med. 2016 Sep;129(9):e211. doi: 10.1016/j.amjmed.2016.04.025. Am J Med. 2016. PMID: 27554963 No abstract available.
References
-
- Steiner C, Andrews R, Barrett M, Weiss A. Report # 2012-03. U.S. Agency for Healthcare Research and Quality; [Accessed November 1, 2014]. HCUP Projections: Mobility/Orthopedic Procedures 2003 to 2012. http://www.hcup-us.ahrq.gov/reports/projections/2012-03.pdf. Published September 20, 2012.
-
- Haralson RH, 3rd, Zuckerman JD. Prevalence, health care expenditures, and orthopedic surgery workforce for musculoskeletal conditions. JAMA. 2009;302:1586–1587. - PubMed
-
- Weiss AJ, Elixhauseer A. HCUP Statistical brief #171. Agency for Healthcare Research and Quality; Rockville, MD: Mar, 2014. Trends in operating room procedures in US Hospitals, 2001–2011.
-
- Seicean A, Seicean S, Alan N, Schiltz NK, Rosenbaum BP, Jones PK, Kattan MW, Neuhauser D, Weil RJ. Preoperative anemia and perioperative outcomes in patients who undergo elective spine surgery. Spine. 2013;38:1331–1341. - PubMed
-
- Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB. An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am. 1999;81:2–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
