

Radiological Evaluation of Bowel Ischemia
- PMID: 26526436
- PMCID: PMC4633709
- DOI: 10.1016/j.rcl.2015.06.009
Radiological Evaluation of Bowel Ischemia
Abstract
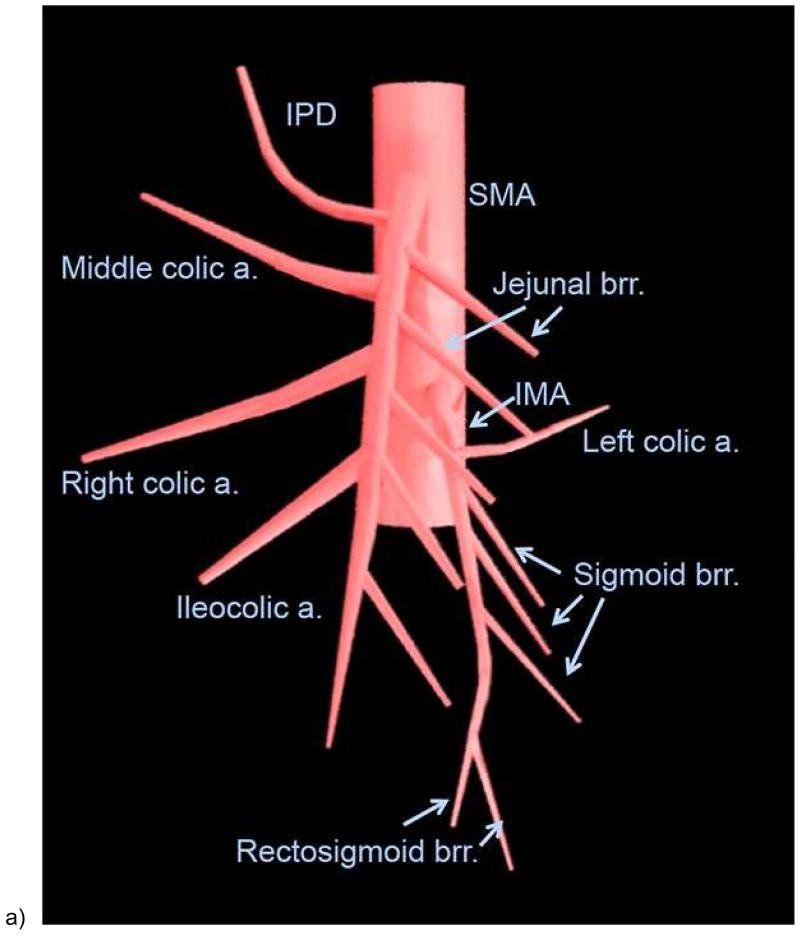
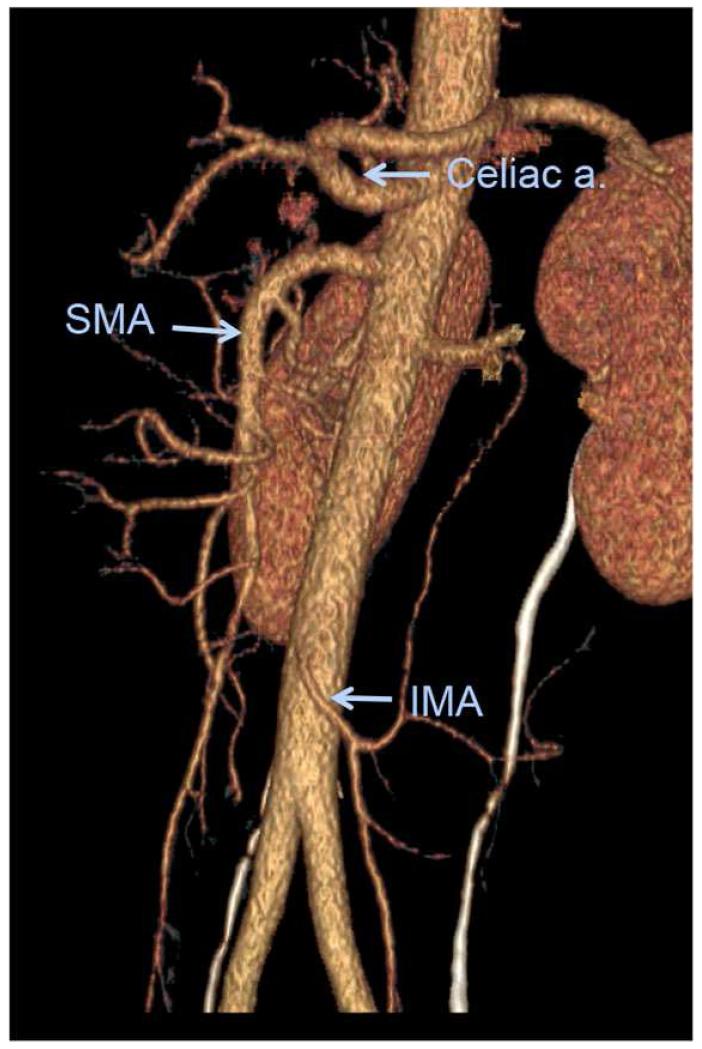
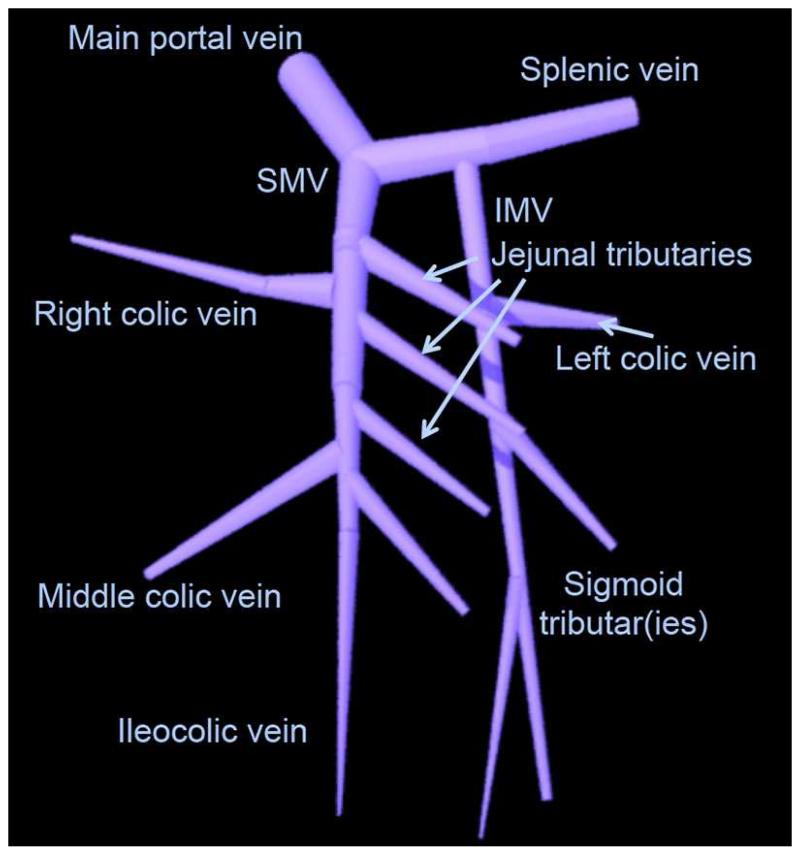
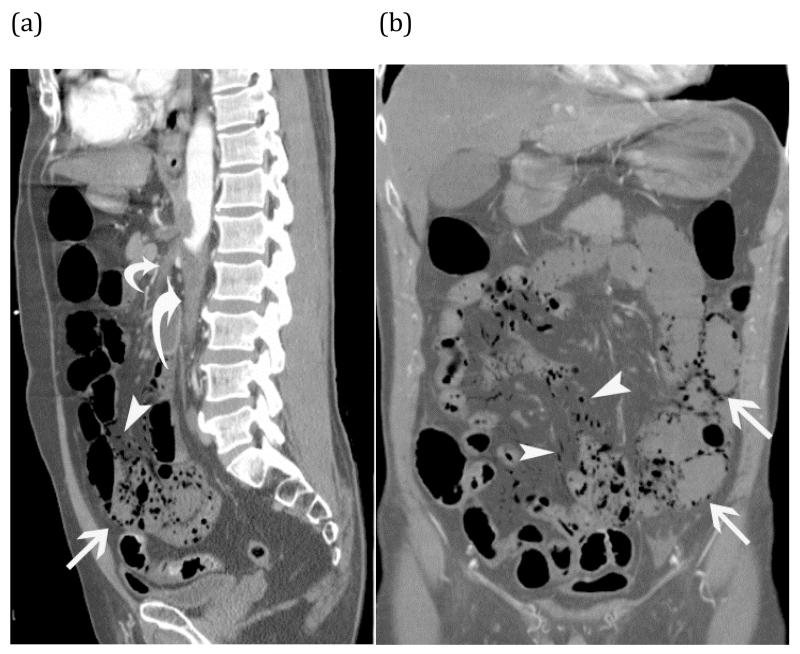
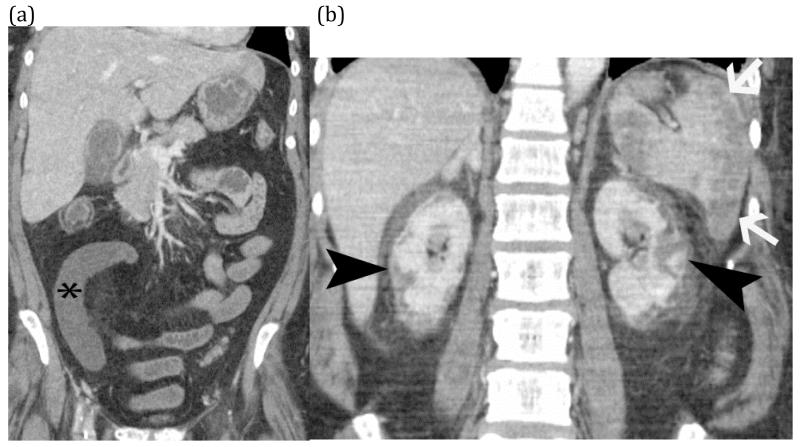
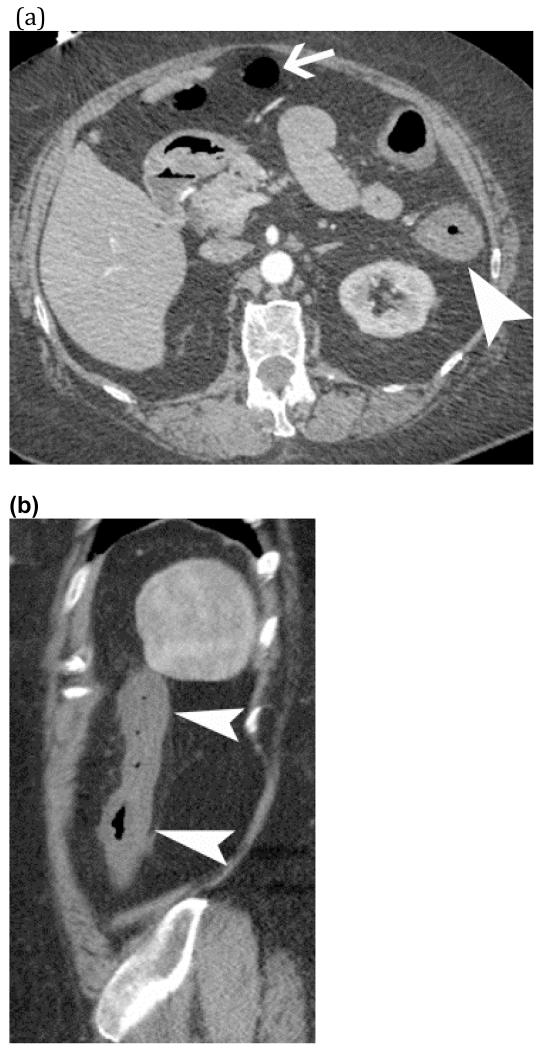
Intestinal ischemia, which refers to insufficient blood flow to the bowel, is a potentially catastrophic entity that may require emergent intervention or surgery in the acute setting. Although the clinical signs and symptoms of intestinal ischemia are nonspecific, computed tomography (CT) findings can be highly suggestive in the correct clinical setting. In our article, we review the CT diagnosis of arterial, venous, and nonocclusive intestinal ischemia. We discuss the vascular anatomy, pathophysiology of intestinal ischemia, CT techniques for optimal imaging, key and ancillary radiological findings, and differential diagnosis.
Keywords: Bowel infarction; Bowel ischemia; Computed tomography; Intestinal ischemia; Mesenteric artery occlusion; Mesenteric ischemia; Oral contrast; Pneumatosis intestinalis.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures




References
-
- Cartwright SL, Knudson MP. Evaluation of acute abdominal pain in adults. American family physician. 2008;77(7):971–8. - PubMed
-
- Ruotolo RA, Evans SR. Mesenteric ischemia in the elderly. Clinics in geriatric medicine. 1999;15(3):527–57. - PubMed
-
- Kumar S, Sarr MG, Kamath PS. Mesenteric venous thrombosis. The New England journal of medicine. 2001;345(23):1683–8. - PubMed
-
- Stamatakos M, Stefanaki C, Mastrokalos D, et al. Mesenteric ischemia: still a deadly puzzle for the medical community. The Tohoku journal of experimental medicine. 2008;216(3):197–204. - PubMed
-
- Huang HH, Chang YC, Yen DH, et al. Clinical factors and outcomes in patients with acute mesenteric ischemia in the emergency department. Journal of the Chinese Medical Association: JCMA. 2005;68(7):299–306. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
