

Paving the Road to Tumor Development and Spreading: Myeloid-Derived Suppressor Cells are Ruling the Fate
- PMID: 26528286
- PMCID: PMC4601280
- DOI: 10.3389/fimmu.2015.00523
Paving the Road to Tumor Development and Spreading: Myeloid-Derived Suppressor Cells are Ruling the Fate
Abstract
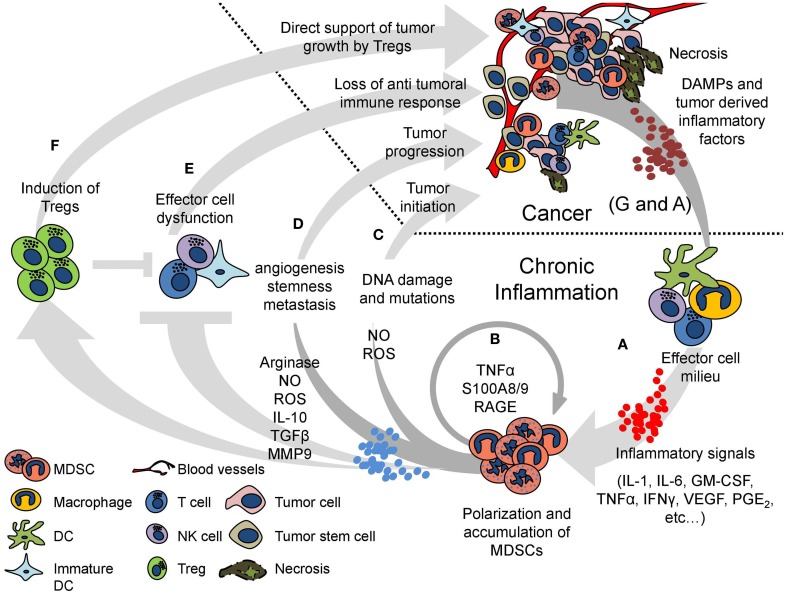
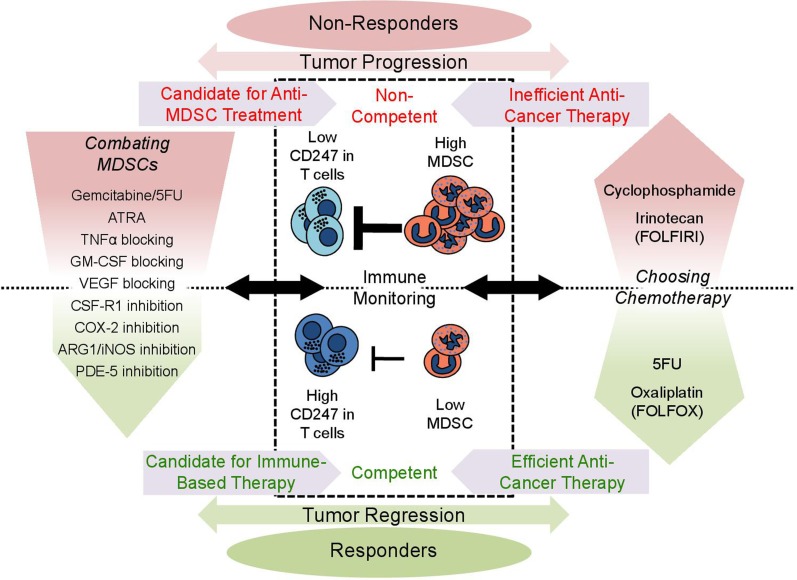
Cancer development is dependent on intrinsic cellular changes as well as inflammatory factors in the tumor macro and microenvironment. The inflammatory milieu nourishes the tumor and contributes to cancer progression. Numerous studies, including ours, have demonstrated that the tumor microenvironment is immunosuppressive, impairing the anticancer immune responses. Chronic inflammation was identified as the key process responsible for this immunosuppression via induction of immature myeloid-derived suppressor cells (MDSCs). Upon a prolonged immune response, MDSCs are polarized toward immunosuppressive cells meant to control the exacerbated immune response. In cancer, the chronic inflammatory response renders the MDSCs harmful. Polarized MDSCs suppress T-cells and natural killer cells, as well as antigen-presenting cells, abrogating the beneficial immune response. These changes in the immunological milieu could also lead to high frequency of mutations, enhanced cancer cell stemness, and angiogenesis, directly supporting tumor initiation, growth, and spreading. The presence of MDSCs in cancer poses a serious obstacle in a variety of immune-based therapies, which rely on the stimulation of antitumor immune responses. Cumulative data, including our own, suggest that the selection of an appropriate and effective anticancer therapy must take into consideration the host's immune status as well as tumor-related parameters. Merging biomarkers for immune monitoring into the traditional patient's categorization and follow-up can provide new predictive and diagnostic tools to the clinical practice. Chronic inflammation and MDSCs could serve as novel targets for therapeutic interventions, which can be combined with conventional cancer treatments such as chemotherapy, radiotherapy, and cancer cell-targeted and immune-based therapies. Intervention in environmental and tumor-specific inflammatory mechanisms will allow better clinical management of cancer toward more efficient treatment.
Keywords: MDSC; biomarkers; cancer; chemotherapy; immune monitoring; immunosuppression; immunotherapy; inflammation.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources