

Using Ambulatory Voice Monitoring to Investigate Common Voice Disorders: Research Update
- PMID: 26528472
- PMCID: PMC4607864
- DOI: 10.3389/fbioe.2015.00155
Using Ambulatory Voice Monitoring to Investigate Common Voice Disorders: Research Update
Abstract
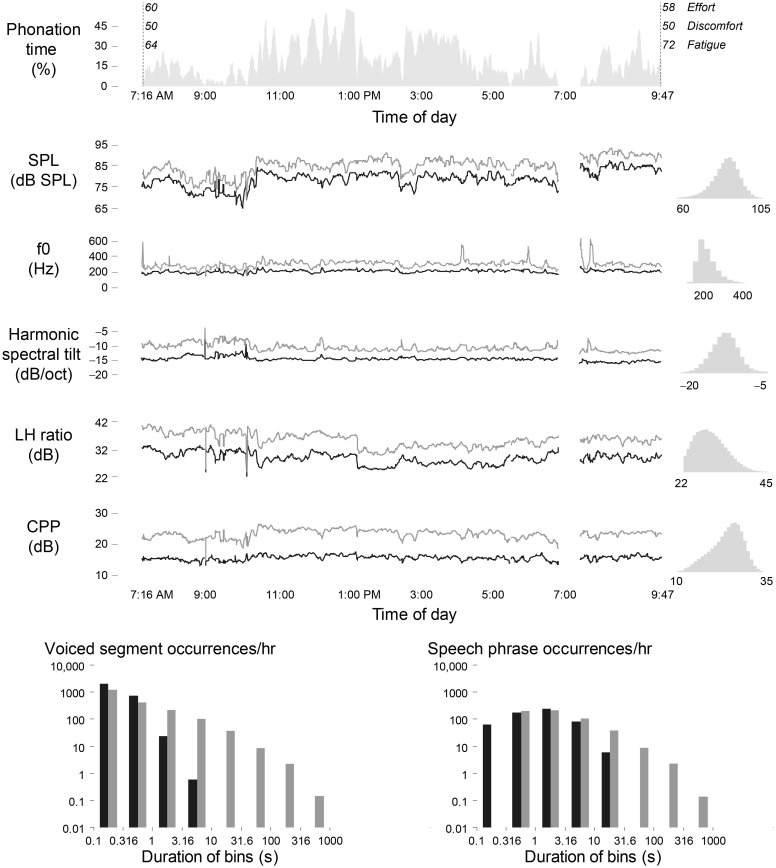
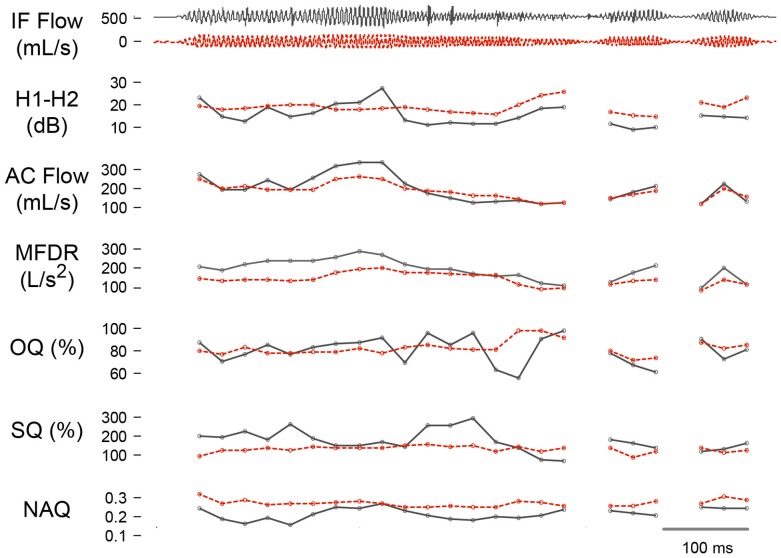
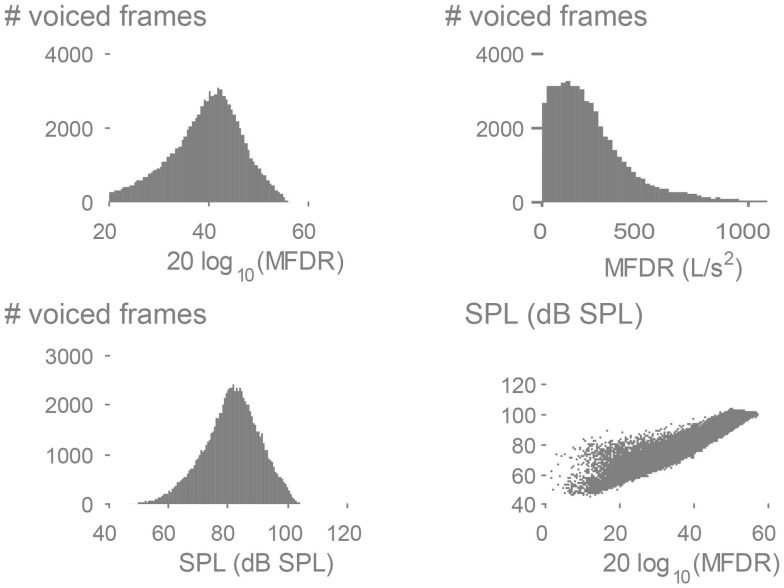
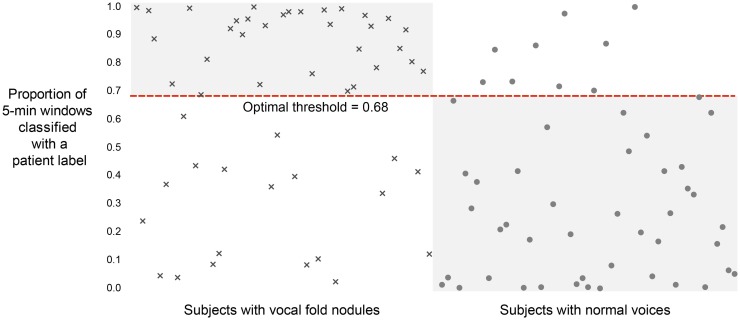
Many common voice disorders are chronic or recurring conditions that are likely to result from inefficient and/or abusive patterns of vocal behavior, referred to as vocal hyperfunction. The clinical management of hyperfunctional voice disorders would be greatly enhanced by the ability to monitor and quantify detrimental vocal behaviors during an individual's activities of daily life. This paper provides an update on ongoing work that uses a miniature accelerometer on the neck surface below the larynx to collect a large set of ambulatory data on patients with hyperfunctional voice disorders (before and after treatment) and matched-control subjects. Three types of analysis approaches are being employed in an effort to identify the best set of measures for differentiating among hyperfunctional and normal patterns of vocal behavior: (1) ambulatory measures of voice use that include vocal dose and voice quality correlates, (2) aerodynamic measures based on glottal airflow estimates extracted from the accelerometer signal using subject-specific vocal system models, and (3) classification based on machine learning and pattern recognition approaches that have been used successfully in analyzing long-term recordings of other physiological signals. Preliminary results demonstrate the potential for ambulatory voice monitoring to improve the diagnosis and treatment of common hyperfunctional voice disorders.
Keywords: accelerometer; glottal inverse filtering; machine learning; vocal function; vocal hyperfunction; voice disorders; voice monitoring.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources