

Laparoscopy-assisted transgastric endoscopic retrograde cholangiopancreatography in bariatric Roux-en-Y gastric bypass patients
- PMID: 26528502
- PMCID: PMC4612229
- DOI: 10.1055/s-0034-1392108
Laparoscopy-assisted transgastric endoscopic retrograde cholangiopancreatography in bariatric Roux-en-Y gastric bypass patients
Abstract
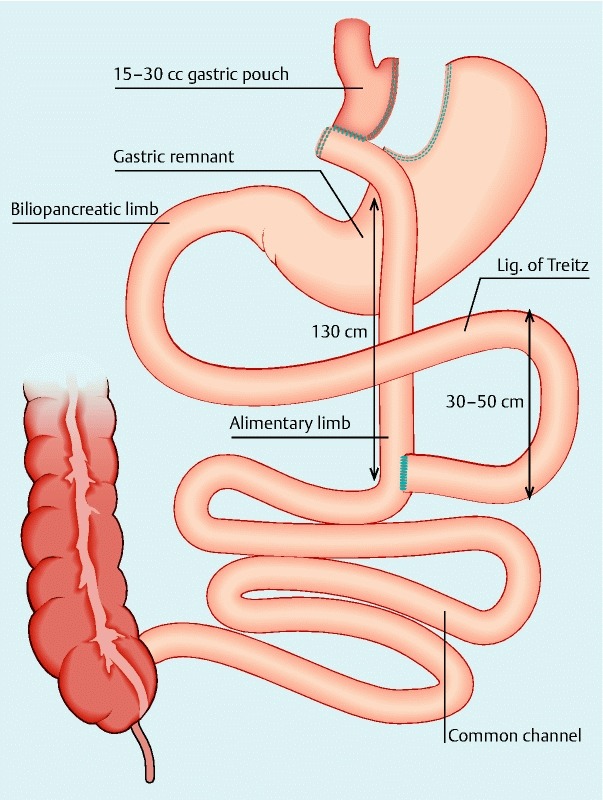
Background: Performing endoscopic retrograde cholangiopancreatography in bariatric patients who underwent Roux-en-Y gastric bypass surgery is challenging due to the long anatomical route required to reach the biliopancreatic limb.
Aim: Assessment of the feasibility and performance of laparoscopy-assisted transgastric endoscopic retrograde cholangiopancreatography.
Methods: A retrospective multicenter observational consecutive-patient cohort study of all patients in the period May 2008 to September 2014 with a history of Roux-en-Y gastric bypass who presented with complicated biliary disease and who underwent a laparoscopy-assisted transgastric endoscopic retrograde cholangiopancreatography. The laparoscopy-assisted transgastric endoscopic retrograde cholangiopancreatography procedure was similar in all centers and was performed through a 15 mm or 18 mm trocar that was inserted in the gastric remnant. Cholecystectomy was performed concomitantly when indicated.
Results: In total, 23 patients underwent a laparoscopy-assisted transgastric endoscopic retrograde cholangiopancreatography procedure. Two patients required a mini-laparotomy for transgastric access because of a complex surgical history resulting in multiple adhesions. Indications included ascending cholangitis, choledocholithiasis, and biliary pancreatitis. Of the 23 patients, 13 underwent concomitant cholecystectomy. All patients successfully underwent biliary cannulation and sphincterotomy. No endoscopic procedure-related complications (i. e. bleeding, pancreatitis or retroperitoneal perforation) occurred. Mean hospital stay was 2.8 days (range 2 - 4).
Conclusions: Transgastric endoscopic retrograde cholangiopancreatography is a feasible approach in the treatment of pancreaticobiliary disease in Roux-en-Y gastric bypass patients, without major complications in our series and allows endoscopic treatment and cholecystectomy to be performed consecutively in a single procedure. In Roux-en-Y gastric bypass patients without a history of prior cholecystectomy presenting with complicated gallstone disease, combining cholecystectomy and transgastric endoscopic retrograde cholangiopancreatography as a first-line approach may be a valid treatment strategy.
Conflict of interest statement
Figures

References
-
- D’Hondt M, Sergeant G, Deylgat B. et al. Prophylactic cholecystectomy, a mandatory step in morbidly obese patients undergoing laparoscopic Roux-en-Y gastric bypass? J Gastrointest Surg. 2011;15:1532–1536. - PubMed
-
- Schreiner M A, Chang L, Gluck M. et al. Laparoscopy-assisted versus balloon enteroscopy-assisted ERCP in bariatric post-Roux-en-Y gastric bypass patients. Gastrointest Endosc. 2012;75:748–756. - PubMed
-
- Aabakken L. Endoscopic retrograde cholangiopancreatography. Gastrointest Endosc. 2012;76:516–520. - PubMed
-
- Lopes T L, Clements R H, Wilcox C M. Laparoscopy-assisted ERCP: experience of a high-volume bariatric surgery center (with video) Gastrointest Endosc. 2009;70:1254–1259. - PubMed
-
- Bertin P M 1, Singh K, Arregui M E. Laparoscopic transgastric endoscopic retrograde cholangiopancreatography (ERCP) after gastric bypass: case series and a description of technique. Surg Endosc. 2011;25:2592–2596. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials