

Tunnel Enlargement and Coalition After Anatomic Double-Bundle Anterior Cruciate Ligament Reconstruction With Hamstring Tendon Autografts: A Computed Tomography Study
- PMID: 26535227
- PMCID: PMC4555502
- DOI: 10.1177/2325967113486441
Tunnel Enlargement and Coalition After Anatomic Double-Bundle Anterior Cruciate Ligament Reconstruction With Hamstring Tendon Autografts: A Computed Tomography Study
Abstract
Background: Tunnel enlargement and coalition following double-bundle anterior cruciate ligament (ACL) reconstruction with hamstring tendon autografts has not yet been sufficiently studied.
Hypothesis: The incidence and the degree of femoral tunnel enlargement will be significantly greater than those for tibial tunnel enlargement after anatomic double-bundle ACL reconstruction using hamstring tendon autografts. There will be no significant correlation between tunnel enlargement and coalition and the postoperative knee laxity.
Study design: Case series; Level of evidence, 4.
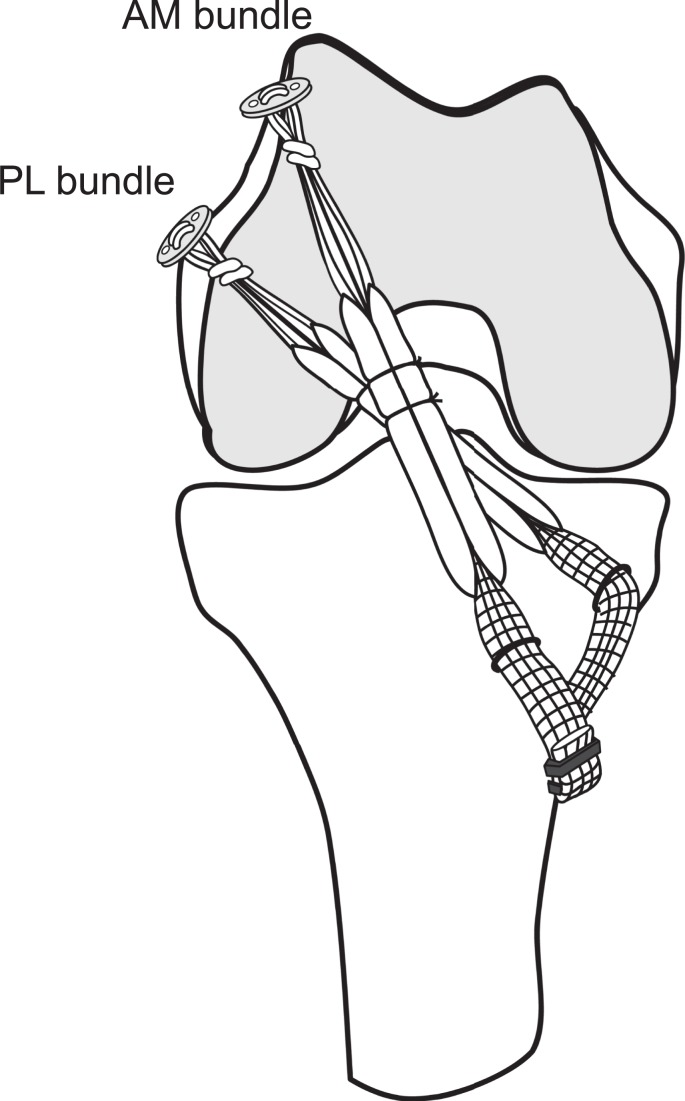
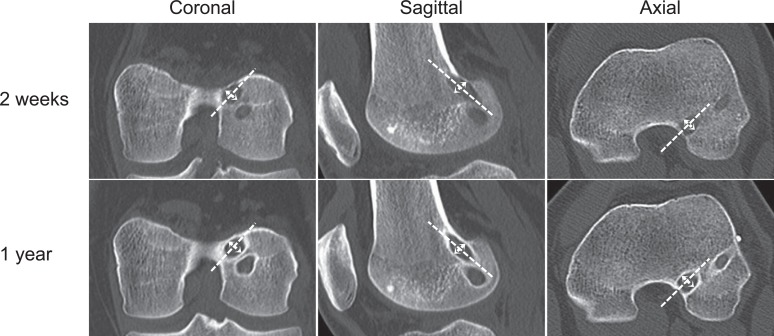
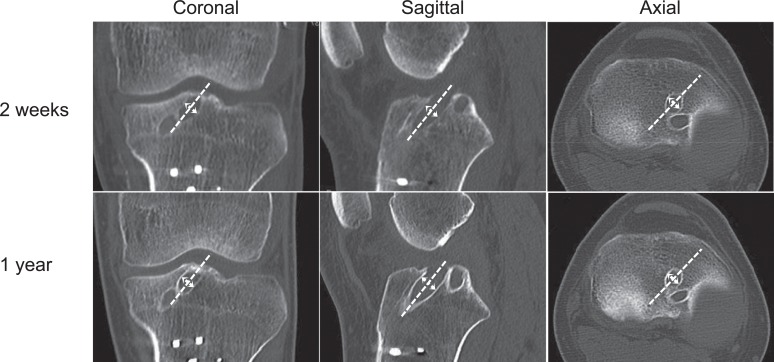
Methods: Thirty-nine patients who underwent anatomic double-bundle ACL reconstruction using semitendinosus and gracilis tendon autografts were followed up for 1 year after surgery. The grafts were simultaneously fixed at 10° of knee flexion with EndoButtons and spiked staples. All patients were examined with computed tomography and the standard clinical evaluation methods at 2 weeks and 1 year after surgery.
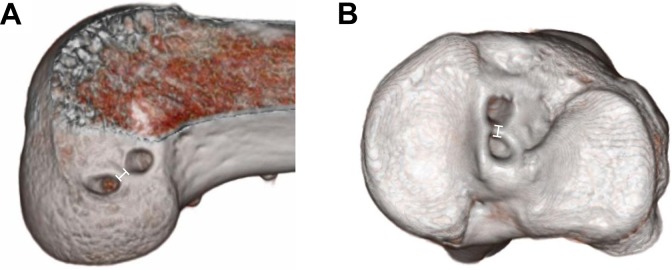
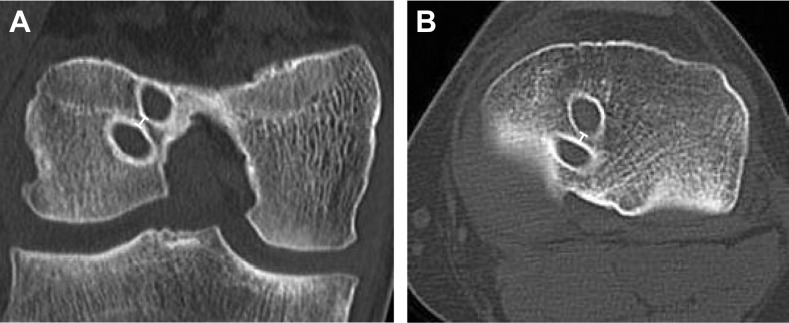
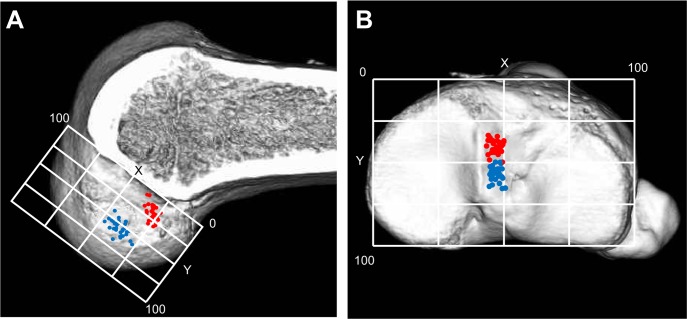
Results: The degree of tunnel enlargement of the femoral anteromedial and posterolateral tunnels averaged 10% to 11% and 7% to 9%, respectively, while that of the tibial anteromedial and posterolateral tunnels averaged 3% to 7% and 1% to 6%. The degree and incidence of the anteromedial and posterolateral tunnel enlargement were significantly greater in the femur than in the tibia (P < .0335 and P < .0405, respectively). On the femoral and tibial intra-articular surface, tunnel outlet coalition was found in 5% and 77% of the knees, respectively, at 1 year after surgery. There was no significant correlation between tunnel enlargement and coalition and the clinical outcome.
Conclusion: The incidence and the degree of each tunnel enlargement in the femur were significantly greater than that in the tibia. However, the incidence of tunnel coalition in the femur was significantly less than that in the tibia after double-bundle ACL reconstruction with a transtibial technique. There was no significant correlation between tunnel enlargement and coalition and the clinical outcome.
Clinical relevance: The present study provides orthopaedic surgeons with important information on double-bundle ACL reconstruction with hamstring tendons.
Keywords: anterior cruciate ligament; clinical outcome; coalition; double-bundle reconstruction; hamstring tendon; tunnel enlargement.
Conflict of interest statement
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Figures
References
-
- Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg. 1997;10(1):14–21. - PubMed
-
- Buelow JU, Siebold R, Ellermann A. A prospective evaluation of tunnel enlargement in anterior cruciate ligament reconstruction with hamstrings: extracortical versus anatomical fixation. Knee Surg Sports Traumatol Arthrosc. 2002;10(2):80–85. - PubMed
-
- Cinar BM, Akpinar S, Hersekli MA, et al. The effects of two different fixation methods on femoral bone tunnel enlargement and clinical results in anterior cruciate ligament reconstruction with hamstring tendon graft [in Turkish]. Acta Orthop Traumatol Turc. 2009;43(6):515–521. - PubMed
-
- Clatworthy MG, Annear P, Bulow JU, Bartlett RJ. Tunnel widening in anterior cruciate ligament reconstruction: a prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc. 1999;7(3):138–145. - PubMed
-
- Edwards A, Bull AMJ, Amis AA. The attachments of the anteromedial and posterolateral fibre bundles of the anterior cruciate ligament. Part 2: femoral attachment. Knee Surg Sports Traumatol Arthrosc. 2008;16(1):29–36. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
