

Anatomy and Histology of the Knee Anterolateral Ligament
- PMID: 26535259
- PMCID: PMC4555517
- DOI: 10.1177/2325967113513546
Anatomy and Histology of the Knee Anterolateral Ligament
Abstract
Background: Reconstruction of the anterior cruciate ligament (ACL) is one of the most common procedures in orthopaedic surgery. However, even with advances in surgical techniques and implants, some patients still have residual anterolateral rotatory laxity after reconstruction. A thorough study of the anatomy of the anterolateral region of the knee is needed.
Purpose: To study the anterolateral region and determine the measurements and points of attachments of the anterolateral ligament (ALL).
Study design: Descriptive laboratory study.
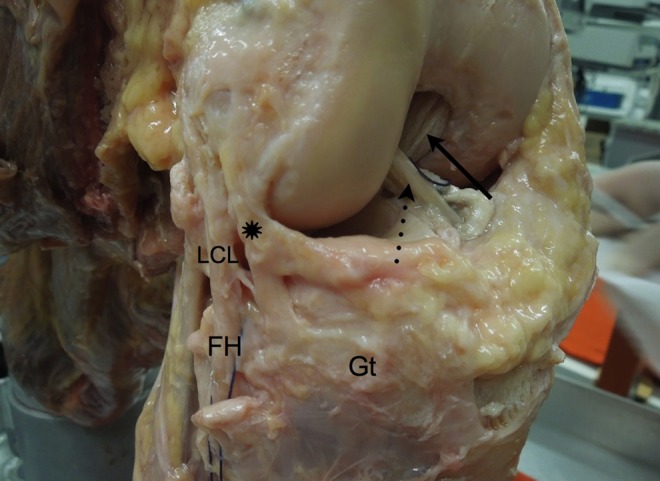
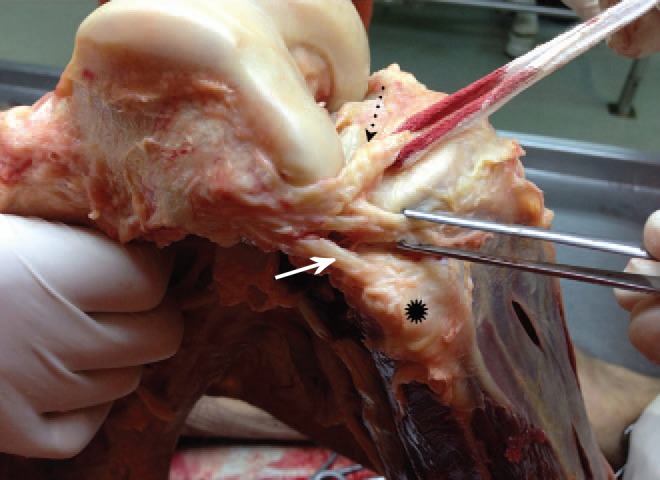
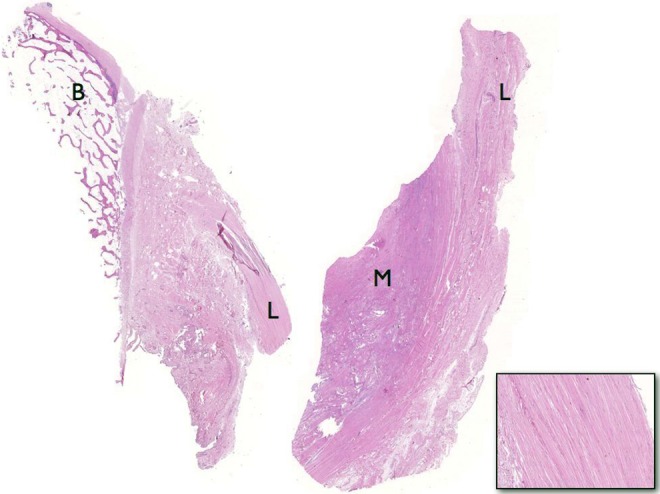
Methods: Dissections of the anterolateral structures of the knee were performed in 20 human cadavers. After isolating the ALL, its length, thickness, width, and points of attachments were determined. The femoral attachment of the ALL was based on the anterior-posterior and proximal-distal distances from the attachment of the lateral collateral ligament (LCL). The tibial attachment point was based on the distance from the Gerdy tubercle to the fibular head and the distance from the lateral tibial plateau. The ligaments from the first 10 dissections were sent for histological analysis.
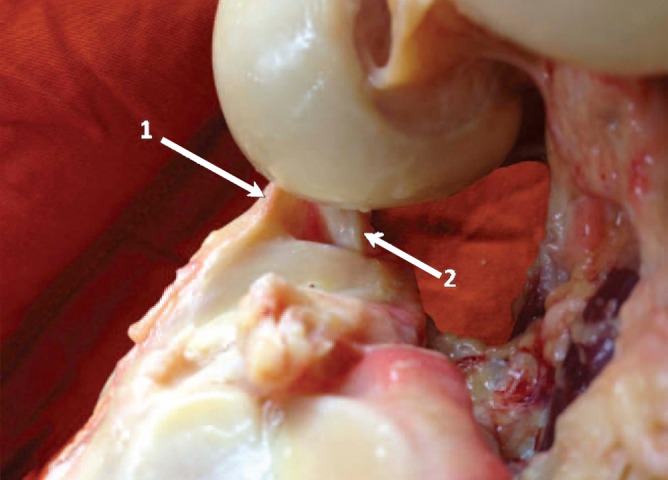
Results: The ALL was found in all 20 knees. The femoral attachment of the ALL at the lateral epicondyle averaged 3.5 mm distal and 2.2 mm anterior to the attachment of the LCL. Two distal attachments were observed: one inserts into the lateral meniscus, the other between the Gerdy tubercle and the fibular head, approximately 4.4 mm distal to the tibial articular cartilage. The mean measurements for the ligament were 37.3 mm (length), 7.4 mm (width), and 2.7 mm (thickness). The histological analysis of the ligaments revealed dense connective tissue.
Conclusion: The ALL is consistently present in the anterolateral region of the knee. Its attachment to the femur is anterior and distal to the attachment of the LCL. Moving distally, it bifurcates at close to half of its length. The ALL features 2 distal attachments, one at the lateral meniscus and the other between the Gerdy tubercle and the fibular head.
Clinical relevance: The ALL may be important in maintaining normal rotatory limits of knee motion; ALL rupture could be responsible for rotatory laxity after isolated intra-articular reconstruction of the ACL.
Keywords: ACL; anatomy; anterolateral ligament; rotatory instability.
Conflict of interest statement
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Figures
References
-
- Camanho GL, Bitar AC, Hernandez AJ, Olivi R. Medial patellofemoral ligament reconstruction: a novel technique using the patellar ligament. Arthroscopy. 2007;23:108.e1–108.e4. - PubMed
-
- Camanho GL, Viegas AdC. Anatomic and arthroscopic study of the medial patellofemoral ligament [in Portuguese]. Acta Ortop Bras. 2003;11:145–149.
-
- Campos JC, Chung CB, Lektrakul N, et al. Pathogenesis of the Segond fracture: anatomic and MR imaging evidence of an iliotibial tract or anterior oblique band avulsion. Radiology. 2001;219:381–386. - PubMed
-
- Frank RM, Verma NN. Graft selection in revision ACL reconstruction In:Bach BR, Jr, Provencher MT, eds. ACL Surgery: How to Get It Right the First Time and What to Do if It Fails. Philadelphia, PA: Elsevier; 2010:217.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
