

Glenohumeral Function of the Long Head of the Biceps Muscle: An Electromyographic Analysis
- PMID: 26535304
- PMCID: PMC4555617
- DOI: 10.1177/2325967114523902
Glenohumeral Function of the Long Head of the Biceps Muscle: An Electromyographic Analysis
Abstract
Background: Optimal treatment of superior labral anterior-posterior (SLAP) tears is controversial, in part because the dynamic role of the long head of the biceps muscle (LHBM) in the glenohumeral joint is unclear. The aim of this study was to determine dynamic LHBM behavior during shoulder activity by studying (1) the electromyographic activity of the LHBM during shoulder motion, (2) the effect of elbow immobilization on this activity, and (3) the effect of a load applied to the distal humerus on this activity.
Hypothesis: The LHBM would not play a significant role in active glenohumeral range of motion.
Study design: Controlled laboratory study.
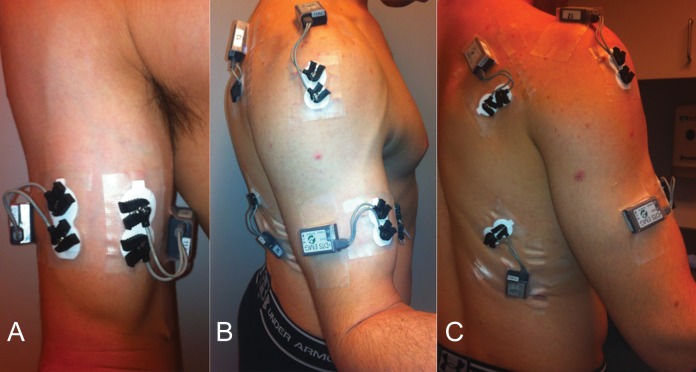
Methods: Thirteen normal volunteers underwent surface electromyography (EMG) measurement of the LHBM, short head biceps muscle (SHBM), deltoid, infraspinatus, and brachioradialis during shoulder motion from the neutral position (0° of rotation, flexion, and abduction) to 45° of flexion, 90° of flexion, 45° of abduction, and 90° of abduction. These motions were repeated both with and without splint immobilization of the forearm and elbow at 100° of flexion and neutral rotation and with and without a 1-kg weight placed on the lateral distal humerus.
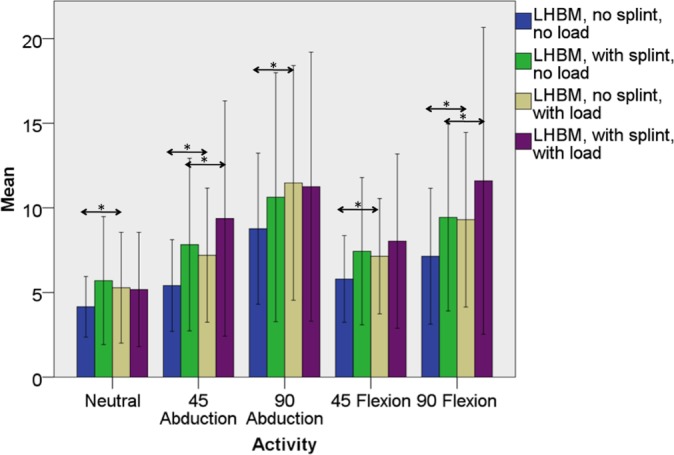
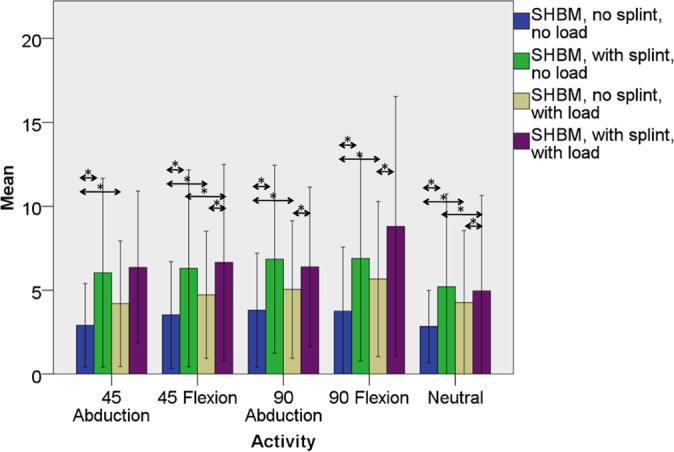
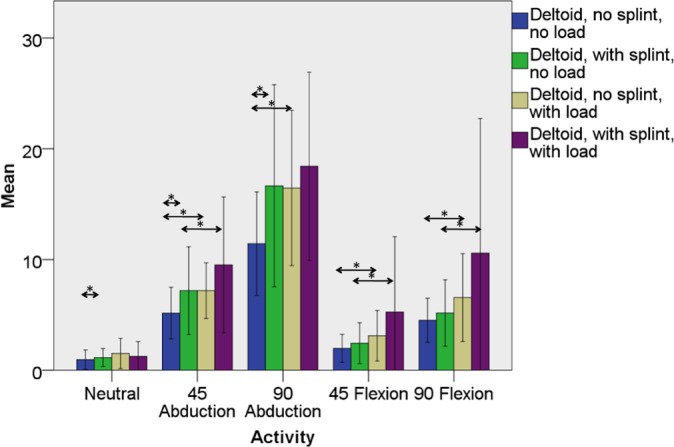
Results: Mean EMG activity within the LHBM and the SHBM was low (≤11.6% ± 9.1%). LHBM activity was significant increased by flexion and abduction (P < .049 in all cases), while SHBM activity was not. EMG activity from the middle head of the deltoid was significantly increased by loading with the shoulder positioned away from the body (ie, in abduction or flexion). When compared with the unloaded state, the addition of a distal humeral load significantly increased LHBM activity in 45° of abduction (P = .028) and 90° of flexion (P = .033) despite forearm and elbow immobilization. The SHBM showed similar trends.
Conclusion: In normal volunteers with forearm and elbow immobilization and application of a load to the distal humerus, LHBM EMG activity is increased by both glenohumeral flexion and abduction, suggesting that this muscle plays a dynamic role in glenohumeral motion with higher demand activities.
Clinical relevance: Biceps tenodesis may result in dynamic change within the glenohumeral joint with higher demand activities.
Keywords: biceps tendon; electromyography; labral tear; long head of biceps tendon; superior labral anterior posterior (SLAP) tear; upper extremity immobilization.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by grants from the Arthroscopy Association of North America and KFx Medical Inc. B.J.C. receives royalties from Arthrex and DJ Orthopaedics; is a paid consultant for Arthrex, DJ Orthopaedics, Johnson & Johnson, Regentis, and Zimmer; has stock or stock options in Carticept and Regentis; receives research support from Johnson & Johnson, Medipost, and Zimmer; receives publication royalties from Elsevier, Lippincott, Smith & Nephew, and WB Saunders; serves on the boards of the American Academy of Orthopaedic Surgery, the
Figures
References
-
- Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009;37:929–936. - PubMed
-
- Brown JM, Solomon C, Paton M. Further evidence of functional differentiation within biceps brachii. Electromyogr Clin Neurophysiol. 1993;33:301–309. - PubMed
-
- Dupont L, Gamet D, Pérot C. Motor unit recruitment and EMG power spectra during ramp contractions of a bifunctional muscle. J Electromyogr Kinesiol. 2000;10:217–224. - PubMed
-
- Hawkes DH, Alizadehkhaiyat O, Fisher AC, Kemp GJ, Roebuck MM, Frostick SP. Normal shoulder muscular activation and co-ordination during a shoulder elevation task based on activities of daily living: an electromyographic study. J Orthop Res. 2011;30:53–60. - PubMed
-
- McMahon PJ, Burkart A, Musahl V, Debski RE. Glenohumeral translations are increased after a type II superior labrum anterior-posterior lesion: a cadaveric study of severity of passive stabilizer injury. J Shoulder Elbow Surg. 2004;13:39–44. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
