

Precision medicine for cancer with next-generation functional diagnostics
- PMID: 26536825
- PMCID: PMC4970460
- DOI: 10.1038/nrc4015
Precision medicine for cancer with next-generation functional diagnostics
Abstract
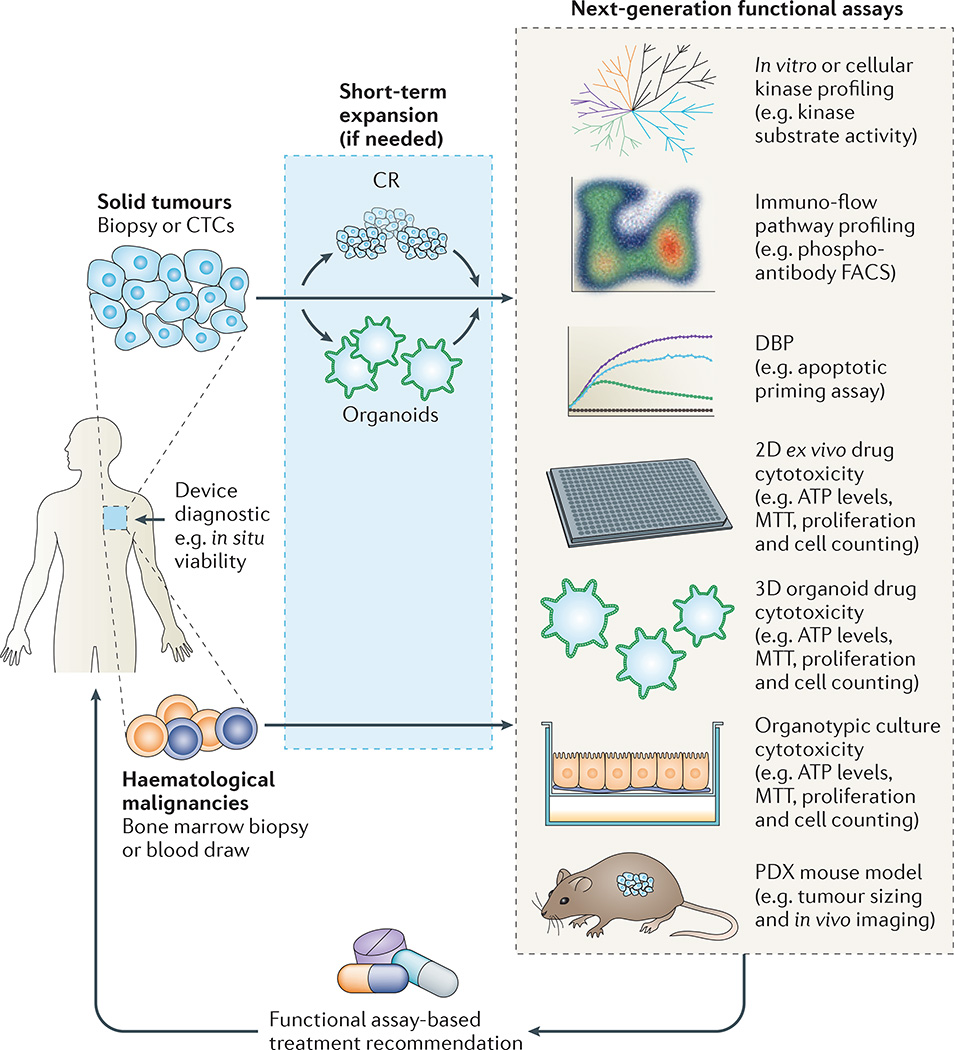
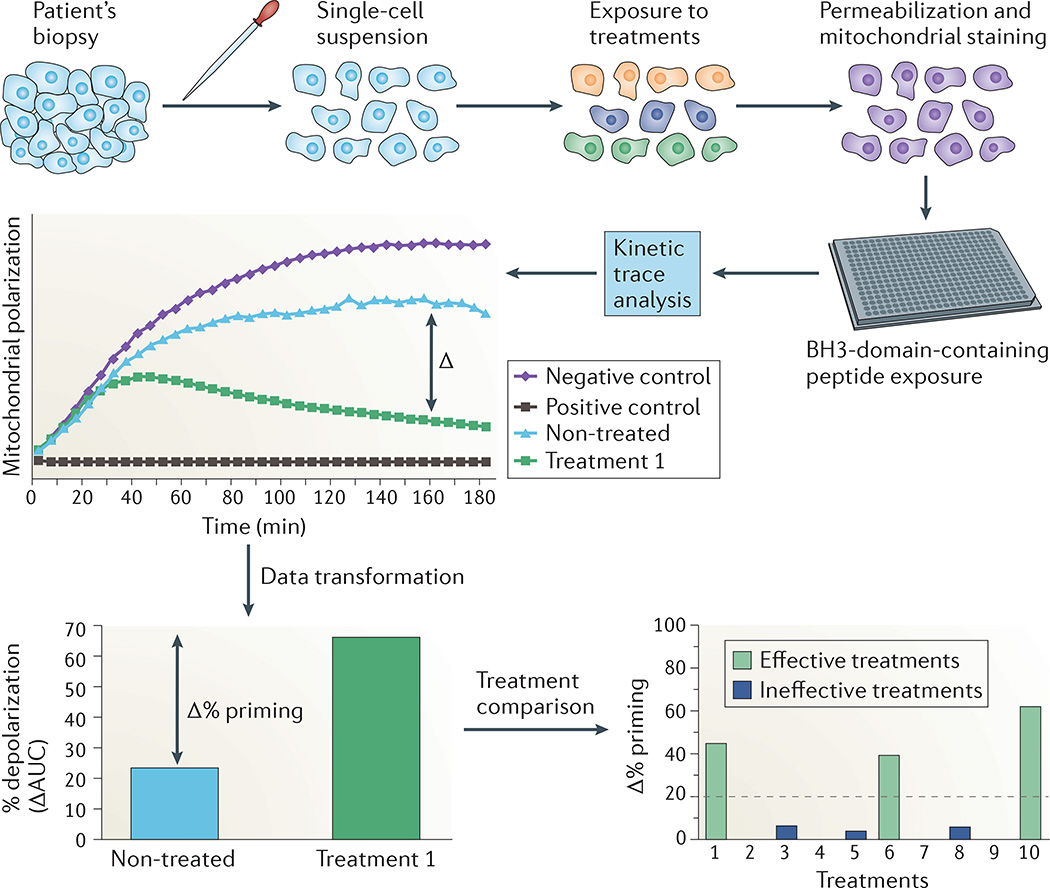
Precision medicine is about matching the right drugs to the right patients. Although this approach is technology agnostic, in cancer there is a tendency to make precision medicine synonymous with genomics. However, genome-based cancer therapeutic matching is limited by incomplete biological understanding of the relationship between phenotype and cancer genotype. This limitation can be addressed by functional testing of live patient tumour cells exposed to potential therapies. Recently, several 'next-generation' functional diagnostic technologies have been reported, including novel methods for tumour manipulation, molecularly precise assays of tumour responses and device-based in situ approaches; these address the limitations of the older generation of chemosensitivity tests. The promise of these new technologies suggests a future diagnostic strategy that integrates functional testing with next-generation sequencing and immunoprofiling to precisely match combination therapies to individual cancer patients.
Figures
References
-
- Sawyers CL, et al. Imatinib induces hematologic and cytogenetic responses in patients with chronic myelogenous leukemia in myeloid blast crisis: results of a Phase II study. Blood. 2002;99:3530–3539. - PubMed
-
- Talpaz M, et al. Imatinib induces durable hematologic and cytogenetic responses in patients with accelerated phase chronic myeloid leukemia: results of a Phase 2 study. Blood. 2002;99:1928–1937. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
