

The impact of comorbid disease history on all-cause and cancer-specific mortality in myeloid leukemia and myeloma - a Swedish population-based study
- PMID: 26537111
- PMCID: PMC4634819
- DOI: 10.1186/s12885-015-1857-x
The impact of comorbid disease history on all-cause and cancer-specific mortality in myeloid leukemia and myeloma - a Swedish population-based study
Abstract
Background: Comorbidity increases overall mortality in patients diagnosed with hematological malignancies. The impact of comorbidity on cancer-specific mortality, taking competing risks into account, has not been evaluated.
Methods: Using the Swedish Cancer Register, we identified patients aged >18 years with a first diagnosis of acute myeloid leukemia (AML, N = 2,550), chronic myeloid leukemia (CML, N = 1,000) or myeloma (N = 4,584) 2002-2009. Comorbid disease history was assessed through in- and out-patient care as defined in the Charlson comorbidity index. Mortality rate ratios (MRR) were estimated through 2012 using Poisson regression. Probabilities of cancer-specific death were computed using flexible parametric survival models.
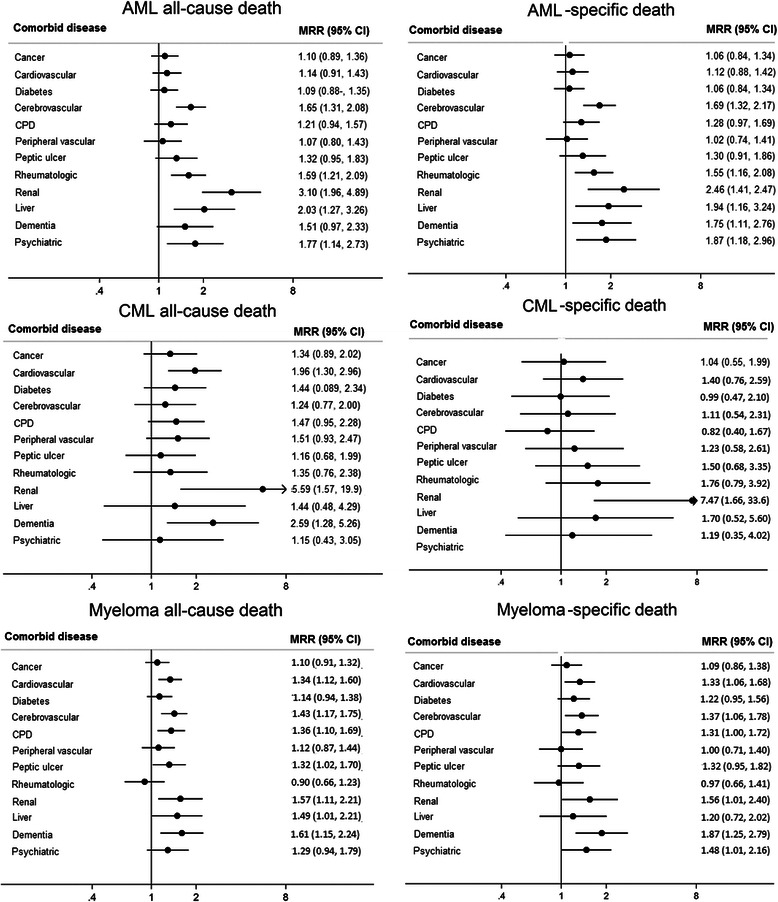
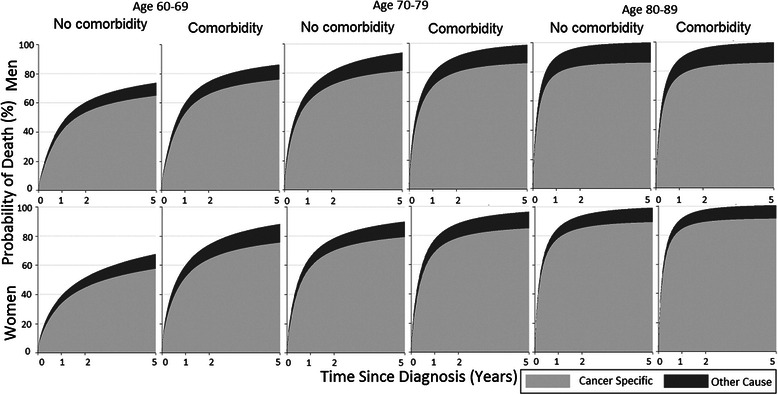
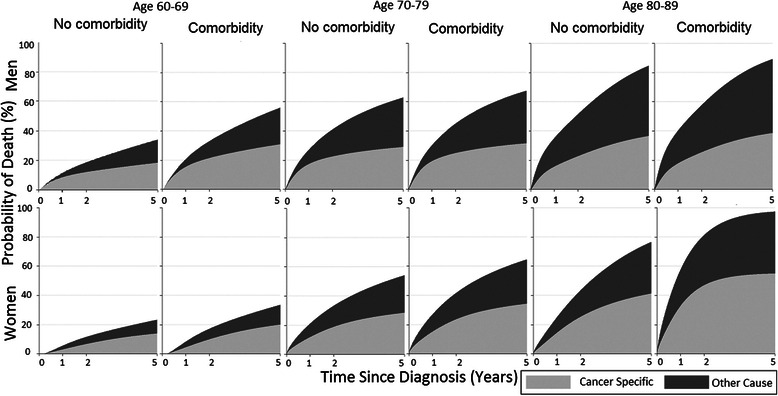
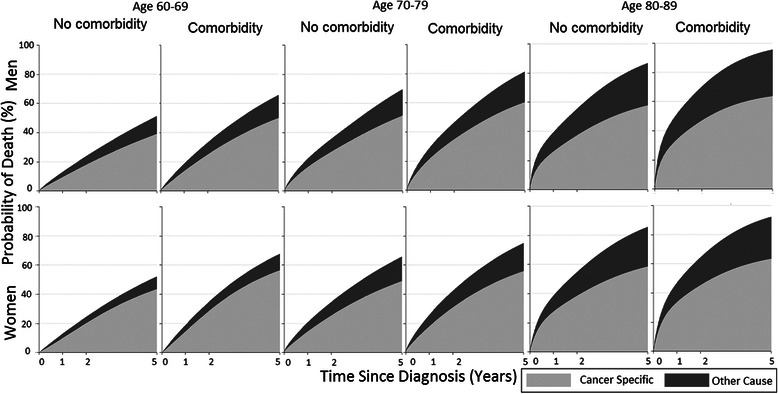
Results: Comorbidity was associated with increased all-cause as well as cancer-specific mortality (cancer-specific MRR: AML = 1.27, 95 % CI: 1.15-1.40; CML = 1.28, 0.96-1.70; myeloma = 1.17, 1.08-1.28) compared with patients without comorbidity. Disorders associated with higher cancer-specific mortality were renal disease (in patients with AML, CML and myeloma), cerebrovascular conditions, dementia, psychiatric disease (AML, myeloma), liver and rheumatic disease (AML), cardiovascular and pulmonary disease (myeloma). The difference in the probability of cancer-specific death, comparing patients with and without comorbidity, was largest among AML patients <70 years, whereas in myeloma the difference did not vary by age among the elderly. The probability of cancer-specific death was generally higher than other-cause death even in older age groups, irrespective of comorbidity.
Conclusion: Comorbidities associated with organ failure or cognitive function are associated with poorer prognosis in several hematological malignancies, likely due to lower treatment tolerability. The results highlight the need for a better balance between treatment toxicity and efficacy in comorbid and elderly AML, CML and myeloma patients.
Figures
References
-
- GLOBOCAN 2012, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 10 [Internet]. [database on the Internet]. Lyon, France: International Agency for Research on Cancer; 2010. Available from: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx, accessed: on 12/06/2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
