

Prolonged prone positioning under VV-ECMO is safe and improves oxygenation and respiratory compliance
- PMID: 26538308
- PMCID: PMC4633431
- DOI: 10.1186/s13613-015-0078-4
Prolonged prone positioning under VV-ECMO is safe and improves oxygenation and respiratory compliance
Abstract
Background: Data are sparse regarding the effects of prolonged prone positioning (PP) during VV-ECMO. Previous studies, using short sessions (<12 h), failed to find any effects on respiratory system compliance. In the present analysis, the effects of prolonged PP sessions (24 h) were retrospectively studied with regard to safety data, oxygenation and respiratory system compliance.
Methods: Retrospective review of 17 consecutive patients who required both VV-ECMO and prone positioning. PP under VV-ECMO was considered when the patient presented at least one unsuccessful ECMO weaning attempt after day 7 or refractory hypoxemia combined or not with persistent high plateau pressure. PP sessions had a duration of 24 h with fixed ECMO and respiratory settings. PP was not performed in patients under vasopressor treatment and in cases of recent open chest cardiac surgery.
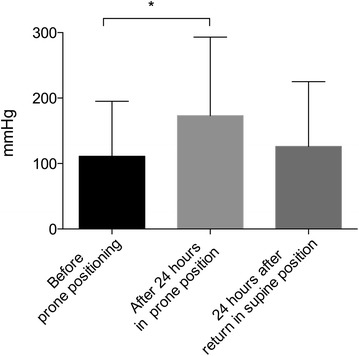
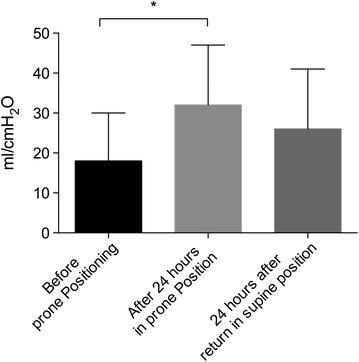
Results: Despite optimized protective mechanical ventilation and other adjuvant treatment (i.e. PP, inhaled nitric oxide, recruitment maneuvers), 44 patients received VV-ECMO during the study period for refractory acute respiratory distress syndrome. Global survival rate was 66 %. Among the latter, 17 patients underwent PP during VV-ECMO for a total of 27 sessions. After 24 h in prone position, PaO2/FiO2 ratio significantly increased from 111 (84-128) to 173 (120-203) mmHg (p < 0.0001) while respiratory system compliance increased from 18 (12-36) to 32 (15-36) ml/cmH2O (p < 0.0001). Twenty-four hours after the return to supine position, tidal volume was increased from 3.0 (2.2-4.0) to 3.7 (2.8-5.0) ml/kg (p < 0.005). PaO2/FiO2 ratio increased by over 20 % in 14/14 sessions for late sessions (≥7 days) and in 7/13 sessions for early sessions (<7 days) (p = 0.01). Quantitative CT scan revealed a high percentage of non-aerated or poorly-aerated lung parenchyma [52 % (41-62)] in all patients. No correlation was found between CT scan data and respiratory parameter changes. Hemodynamics did not vary and side effects were rare (one membrane thrombosis and one drop in ECMO blood flow).
Conclusion: When used in combination with VV-ECMO, 24 h of prone positioning improves both oxygenation and respiratory system compliance. Moreover, our study confirms the absence of serious adverse events.
Keywords: ARDS; ECMO; Prone positioning.
Figures
References
-
- Guerin C, Reignier J, Richard JC, Beuret P, Gacouin A, Boulain T, Mercier E, Badet M, Mercat A, Baudin O, Clavel M, Chatellier D, Jaber S, Rosselli S, Mancebo J, Sirodot M, Hilbert G, Bengler C, Richecoeur J, Gainnier M, Bayle F, Bourdin G, Leray V, Girard R, Baboi L, Ayzac L, Group PS Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159–2168. doi: 10.1056/NEJMoa1214103. - DOI - PubMed
-
- Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, Hibbert CL, Truesdale A, Clemens F, Cooper N, Firmin RK, Elbourne D. CESAR trial collaboration. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009;374:1351–1363. doi: 10.1016/S0140-6736(09)61069-2. - DOI - PubMed
-
- Schmidt M, Zogheib E, Roze H, Repesse X, Lebreton G, Luyt CE, Trouillet JL, Brechot N, Nieszkowska A, Dupont H, Ouattara A, Leprince P, Chastre J, Combes A. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med. 2013;39:1704–1713. doi: 10.1007/s00134-013-3037-2. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
