

Antimicrobial de-escalation of treatment for healthcare-associated pneumonia within the Veterans Healthcare Administration
- PMID: 26538501
- PMCID: PMC4710212
- DOI: 10.1093/jac/dkv338
Antimicrobial de-escalation of treatment for healthcare-associated pneumonia within the Veterans Healthcare Administration
Abstract
Objectives: The objective of this study was to measure quantitatively antimicrobial de-escalation utilizing electronic medication administration data based on the spectrum of activity for antimicrobial therapy (i.e. spectrum score) to identify variables associated with de-escalation in a nationwide healthcare system.
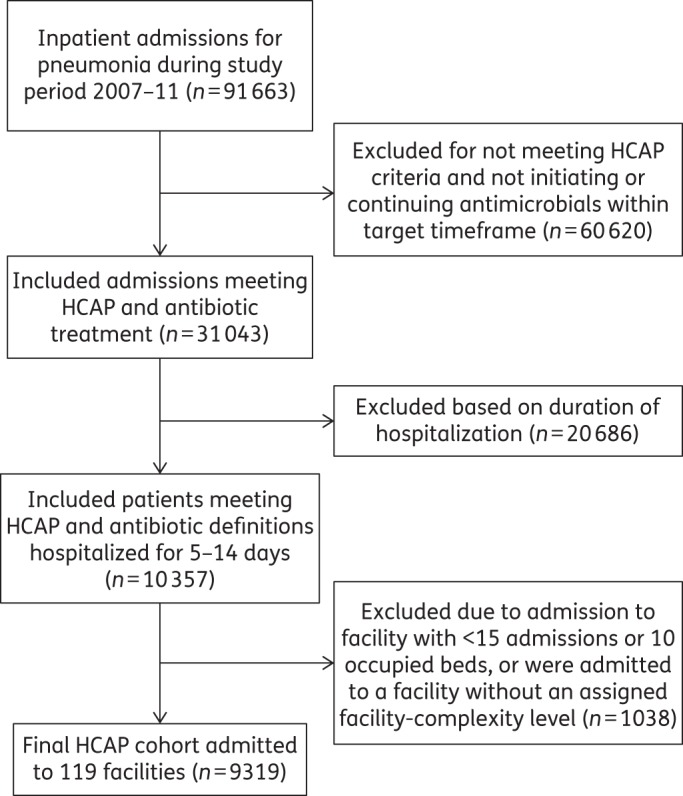
Methods: A retrospective cohort study of patients hospitalized for healthcare-associated pneumonia was conducted in Veterans Affairs Medical Centers (n = 119). Patients hospitalized for healthcare-associated pneumonia on acute-care wards between 5 and 14 days who received antimicrobials for ≥ 3 days during calendar years 2008-11 were evaluated. The spectrum score method was applied at the patient level to measure de-escalation on day 4 of hospitalization. De-escalation was expressed in aggregate and facility-level proportions. Logistic regression was used to assess variables associated with de-escalation. ORs with 95% CIs were reported.
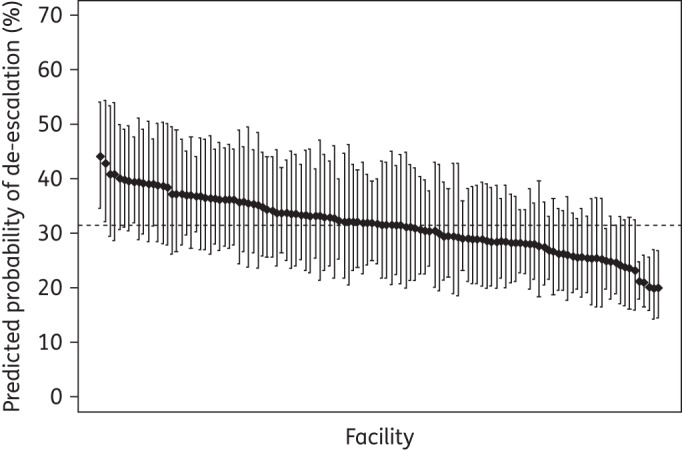
Results: Among 9319 patients, the de-escalation proportion was 28.3% (95% CI 27.4-29.2), which varied 6-fold across facilities [median (IQR) facility-level de-escalation proportion 29.1% (95% CI 21.7-35.6)]. Variables associated with de-escalation included initial broad-spectrum therapy (OR 1.5, 95% CI 1.4-1.5 for each 10% increase in spectrum), collection of respiratory tract cultures (OR 1.1, 95% CI 1.0-1.2) and care in higher complexity facilities (OR 1.3, 95% CI 1.1-1.6). Respiratory tract cultures were collected from 35.3% (95% CI 32.7-37.7) of patients.
Conclusions: De-escalation of antimicrobial therapy was limited and varied substantially across facilities. De-escalation was associated with respiratory tract culture collection and treatment in a high complexity-level facility.
© The Author 2015. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Promoting Antimicrobial Stewardship in Human Medicine. http://www.idsociety.org/Stewardship_Policy/.
-
- American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005; 171: 388–416. - PubMed
-
- Dellit TH, Owens RC, McGowan JE Jr et al. . Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis 2007; 44: 159–77. - PubMed
-
- Society for Healthcare Epidemiology of America, Infectious Diseases Society of America, Pediatric Infectious Diseases Society. Policy statement on antimicrobial stewardship by the Society for Healthcare Epidemiology of America (SHEA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS). Infect Control Hosp Epidemiol 2012; 33: 322–77. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
