

Next-Generation Testing for Cancer Risk: Perceptions, Experiences, and Needs Among Early Adopters in Community Healthcare Settings
- PMID: 26539620
- PMCID: PMC4677543
- DOI: 10.1089/gtmb.2015.0061
Next-Generation Testing for Cancer Risk: Perceptions, Experiences, and Needs Among Early Adopters in Community Healthcare Settings
Abstract
Background: Advances in next-generation sequencing (NGS) technologies are driving a shift from single-gene to multigene panel testing for clinical genetic cancer risk assessment (GCRA). This study explored perceptions, experiences, and challenges with NGS testing for GCRA among U.S. community-based clinicians.
Methods: Surveys delivered at initial and 8-month time points, and 12-month tracking of cases presented in a multidisciplinary web-based case conference series, were conducted with GCRA providers who participated in a 235-member nationwide community of practice.
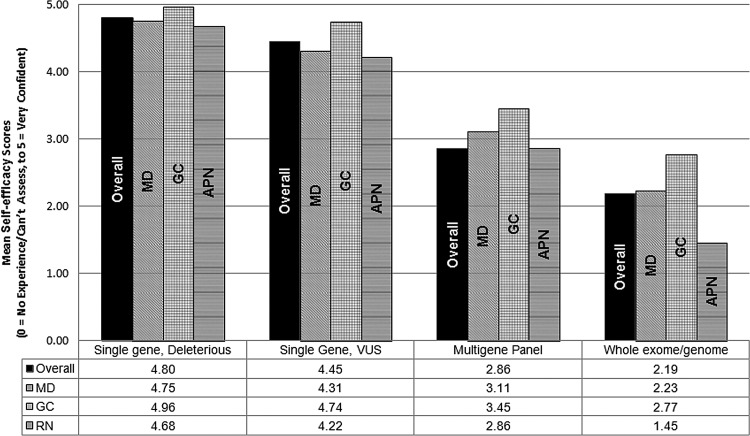
Results: The proportion of respondents ordering panel tests rose from 29% at initial survey (27/94) to 44% (46/107) within 8 months. Respondents reported significantly less confidence about interpreting and counseling about NGS compared with single-gene test results (p < 0.0001 for all comparisons). The most cited reasons for not ordering NGS tests included concerns about clinical utility, interpreting and communicating results, and lack of knowledge/skills. Multigene panels were used in 204/668 cases presented during 2013, yielding 37 (18%) deleterious (7% in low/moderate-penetrance genes), 88 (43%) with ≥1 variant of uncertain significance, 77 (38%) uninformative negative, and 2 (1%) inconclusive results.
Conclusions: Despite concerns about utility and ability to interpret/counsel about NGS results, a rapidly increasing uptake of NGS testing among community clinicians was documented. Challenges identified in case discussions point to the need for ongoing education, practice-based support, and opportunities to partner in research that contributes to characterization of lesser known genes.
Figures



References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
