

Preventing ICU Subsyndromal Delirium Conversion to Delirium With Low-Dose IV Haloperidol: A Double-Blind, Placebo-Controlled Pilot Study
- PMID: 26540397
- PMCID: PMC4779647
- DOI: 10.1097/CCM.0000000000001411
Preventing ICU Subsyndromal Delirium Conversion to Delirium With Low-Dose IV Haloperidol: A Double-Blind, Placebo-Controlled Pilot Study
Abstract
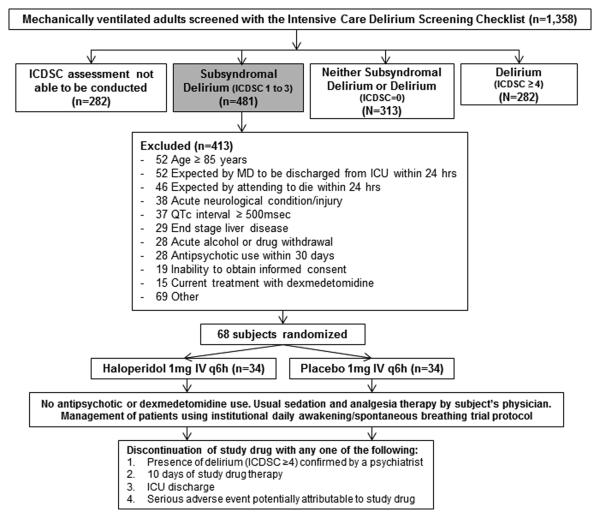
Objective: To compare the efficacy and safety of scheduled low-dose haloperidol versus placebo for the prevention of delirium (Intensive Care Delirium Screening Checklist ≥ 4) administered to critically ill adults with subsyndromal delirium (Intensive Care Delirium Screening Checklist = 1-3).
Design: Randomized, double-blind, placebo-controlled trial.
Setting: Three 10-bed ICUs (two medical and one surgical) at an academic medical center in the United States.
Patients: Sixty-eight mechanically ventilated patients with subsyndromal delirium without complicating neurologic conditions, cardiac surgery, or requiring deep sedation.
Interventions: Patients were randomly assigned to receive IV haloperidol 1 mg or placebo every 6 hours until delirium occurred (Intensive Care Delirium Screening Checklist ≥ 4 with psychiatric confirmation), 10 days of therapy had elapsed, or ICU discharge.
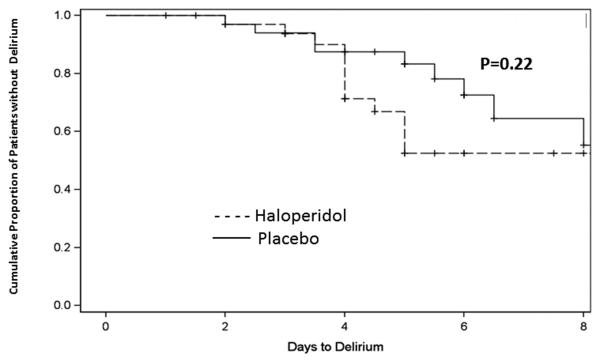
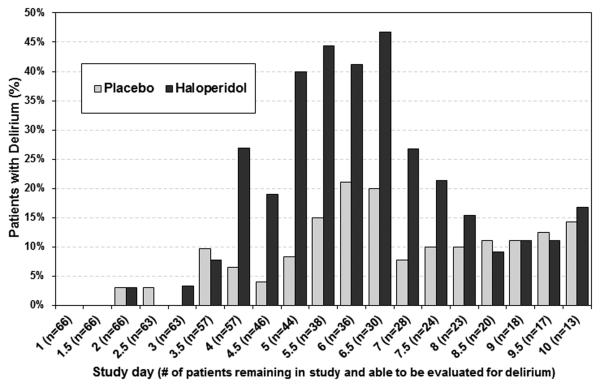
Measurements and main results: Baseline characteristics were similar between the haloperidol (n = 34) and placebo (n = 34) groups. A similar number of patients given haloperidol (12/34 [35%]) and placebo (8/34 [23%]) developed delirium (p = 0.29). Haloperidol use reduced the hours per study day spent agitated (Sedation Agitation Scale ≥ 5) (p = 0.008), but it did not influence the proportion of 12-hour ICU shifts patients spent alive without coma (Sedation Agitation Scale ≤ 2) or delirium (p = 0.36), the time to first delirium occurrence (p = 0.22), nor delirium duration (p = 0.26). Days of mechanical ventilation (p = 0.80), ICU mortality (p = 0.55), and ICU patient disposition (p = 0.22) were similar in the two groups. The proportion of patients who developed corrected QT-interval prolongation (p = 0.16), extrapyramidal symptoms (p = 0.31), excessive sedation (p = 0.31), or new-onset hypotension (p = 1.0) that resulted in study drug discontinuation was comparable between the two groups.
Conclusions: Low-dose scheduled haloperidol, initiated early in the ICU stay, does not prevent delirium and has little therapeutic advantage in mechanically ventilated, critically ill adults with subsyndromal delirium.
Figures
Comment in
-
Early Identification of Subsyndromal Delirium in the Critically Ill: Don't Let the Delirium Rise!Crit Care Med. 2016 Mar;44(3):644-5. doi: 10.1097/CCM.0000000000001544. Crit Care Med. 2016. PMID: 26901554 No abstract available.
-
Mechanistically, How Does Postoperative Delirium Differ From Critical Illness Delirium?Crit Care Med. 2016 Oct;44(10):e1019-20. doi: 10.1097/CCM.0000000000001890. Crit Care Med. 2016. PMID: 27635520 No abstract available.
References
-
- Dubois MJ, Bergeron N, Dumont M, et al. Delirium in an intensive care unit: a study of risk factors. Intensive Care Med. 2001;27:1297–1304. - PubMed
-
- Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291:1753–1762. - PubMed
-
- van den Boogaard M, Schoonhoven L, Evers AW, et al. Delirium in critically ill patients: impact on long-term health-related quality of life and cognitive functioning. Crit Care Med. 2012;40:112–118. - PubMed
-
- Ouimet S, Riker R, Bergeron N. Subsyndromal delirium in the ICU: evidence for a disease spectrum. Intensive Care Med. 2007;33:1007–1113. - PubMed
-
- Bergeron N, Dubois MJ, Dumont M, et al. Intensive Care Delirium Screening Checklist: evaluation of a new screening tool. Intensive Care Med. 2001;27:859–864. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
