

A Dysregulated Balance of Proinflammatory and Anti-Inflammatory Host Cytokine Response Early During Therapy Predicts Persistence and Mortality in Staphylococcus aureus Bacteremia
- PMID: 26540400
- PMCID: PMC6504958
- DOI: 10.1097/CCM.0000000000001465
A Dysregulated Balance of Proinflammatory and Anti-Inflammatory Host Cytokine Response Early During Therapy Predicts Persistence and Mortality in Staphylococcus aureus Bacteremia
Abstract
Objectives: The contribution of individual immune response to Staphylococcus aureus bacteremia on outcome has not been well studied. The objective was to relate the host cytokine response to outcome of Staphylococcus aureus bacteremia.
Design: Prospective observational study.
Setting: Three U.S. university-affiliated medical centers.
Patients: Adult patients infected with Staphylococcus aureus bacteremia hospitalized between July 2012 and August 2014.
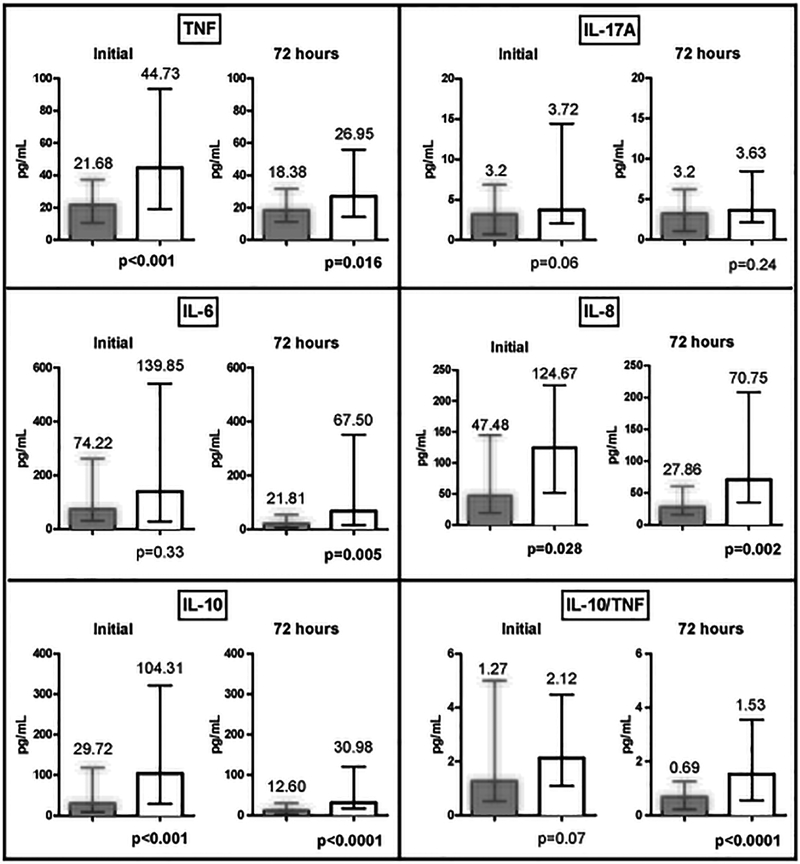
Interventions: Blood specimens were obtained at Staphylococcus aureus bacteremia onset and 72 hours after therapy initiation. Levels of tissue necrosis factor, interleukin-6, interleukin-8, interleukin-17A, and interleukin-10 were measured by enzyme-linked immunosorbent assay at each time point and compared between those with persistent bacteremia (≥ 4 d) and resolving bacteremia. Primary outcome was persistent bacteremia after 4 days of effective therapy. Secondary outcomes were 30-day mortality and 30-day recurrence.
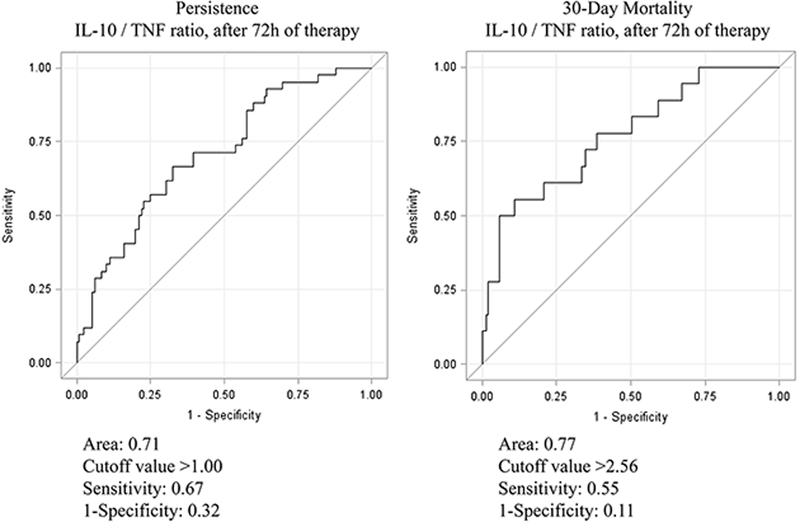
Measurements and main results: A total of 196 patients were included (mean age, 59 yr); of them, 33% had methicillin-resistant Staphylococcus aureus bacteremia. Forty-seven percent of the methicillin-resistant Staphylococcus aureus strains were staphylococcal cassette chromosome mec IV. Persistent bacteremia occurred in 24% of patients (47/196); they were more likely to die than resolving bacteremia group (28% vs 5%; p < 0.001). Compared with resolving bacteremia group, persistent bacteremia patients had higher initial median levels of tissue necrosis factor (44.73 vs 21.68 pg/mL; p < 0.001), interleukin-8 (124.76 vs 47.48 pg/mL; p = 0.028), and interleukin-10 (104.31 vs 29.72 pg/mL; p < 0.001). Despite 72 hours of treatment, levels remained higher for the persistent bacteremia group than for the resolving bacteremia group (tissue necrosis factor: 26.95 vs 18.38 pg/mL, p = 0.02; interleukin-8: 70.75 vs 27.86 pg/mL, p = 0.002; interleukin-6: 67.50 vs 21.81 pg/mL, p = 0.005; and interleukin-10: 30.98 vs 12.60 pg/mL, p < 0.001). Interleukin-17A levels were similar between groups at both time points. After controlling for confounding variables by multivariate analysis, interleukin-10/tissue necrosis factor ratio at 72 hours most significantly predicted persistence (odds ratio, 2.98; 95% CI, 1.39-6.39; p = 0.005) and mortality (odds ratio, 9.87; 95% CI, 2.64-36.91; p < 0.001) at values more than 1.00 and more than 2.56, respectively.
Conclusions: Sustained elevation of interleukin-10/tissue necrosis factor ratio at 72 hours suggests a dysregulated immune response and may be used to guide management to improve outcomes.
Conflict of interest statement
No conflicts of interest for all authors.
Figures
Comment in
-
Cytokine Imbalance Predicts Poor Outcomes in Staphylococcus aureus Bacteremia--But What Can We Do About It?Crit Care Med. 2016 Apr;44(4):846-7. doi: 10.1097/CCM.0000000000001502. Crit Care Med. 2016. PMID: 26974448 No abstract available.
References
-
- Lamagni TL, Potz N, Powell D, et al. Mortality in patients with meticillin-resistant Staphylococcus aureus bacteraemia, England 2004–2005. J Hosp Infect 2011;77(1):16–20. - PubMed
-
- Yoon YK, Kim JY, Park DW, et al. Predictors of persistent methicillin-resistant Staphylococcus aureus bacteraemia in patients treated with vancomycin. J Antimicrob Chemother 2010;65(5):1015–1018. - PubMed
-
- Soriano A, Marco F, Martínez JA, et al. Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Clin Infect Dis 2008;46(2):193–200. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
