

Predicting vision gains with anti-VEGF therapy in neovascular age-related macular degeneration patients by using low-luminance vision
- PMID: 26541435
- PMCID: PMC4975848
- DOI: 10.1136/bjophthalmol-2015-307575
Predicting vision gains with anti-VEGF therapy in neovascular age-related macular degeneration patients by using low-luminance vision
Abstract
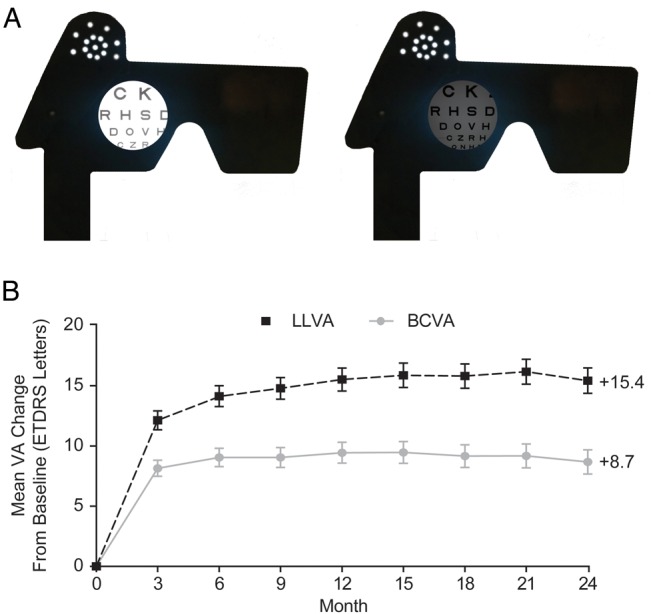
Background/aims: To evaluate baseline low-luminance visual acuity (LLVA) as a predictor of visual acuity improvement in patients with neovascular (wet) age-related macular degeneration (wAMD) receiving antivascular endothelial growth factor A (anti-VEGF) therapy.
Methods: In the HARBOR trial, 1084 treatment-naïve patients ≥50 years of age with subfoveal wAMD received intravitreal ranibizumab 0.5 or 2.0 mg monthly or as needed. To measure LLVA, patients read a normally illuminated ETDRS (Early Treatment Diabetic Retinopathy Study) chart with a neutral density filter placed in front of the study eye. Patients were assigned into quartiles based on the magnitude of the difference between best-corrected visual acuity under optimal luminance (BCVA) and LLVA (BCVA-LLVA gap). The association between mean change in BCVA from baseline and BCVA-LLVA gap at baseline was analysed using a general linear model.
Results: A smaller baseline BCVA-LLVA gap predicted significantly higher BCVA gains over 24 months (p<0.0001 at each month; Pearson correlation), even after controlling for baseline BCVA or stratifying by treatment arm. Patients in the smallest baseline BCVA-LLVA gap quartile gained an average of +13.4 letters compared with +2.4 letters for patients in the widest baseline BCVA-LLVA gap quartile. At months 12 and 24, the smallest baseline BCVA-LLVA gap quartile had the highest proportion of ≥15-≥30-letter gain, and the widest baseline BCVA-LLVA gap quartile had the highest proportion of ≥15-/≥30-letter loss (p<0.0001; Fisher's exact test).
Conclusions: The baseline BCVA-LLVA gap is a significant predictor of visual acuity response to anti-VEGF treatment in patients with wAMD.
Trial registration number: NCT00891735; Post-results.
Keywords: Degeneration; Drugs; Macula; Neovascularisation; Vision.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures



References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous