

Feasibility and clinical impact of sharing patient-reported symptom toxicities and performance status with clinical investigators during a phase 2 cancer treatment trial
- PMID: 26542025
- PMCID: PMC5228492
- DOI: 10.1177/1740774515615540
Feasibility and clinical impact of sharing patient-reported symptom toxicities and performance status with clinical investigators during a phase 2 cancer treatment trial
Abstract
Background: Clinicians can miss up to half of patients' symptomatic toxicities in cancer clinical trials and routine practice. Although patient-reported outcome questionnaires have been developed to capture this information, it is unclear whether clinicians will make use of patient-reported outcomes to inform their own toxicity documentation, or to prompt symptom management activities.
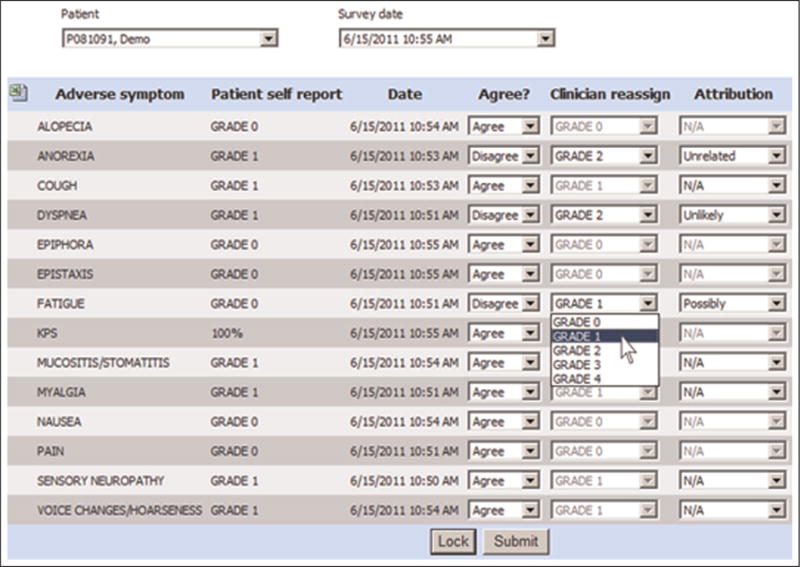
Methods: 44 lung cancer patients that participated in a phase 2 treatment trial self-reported 13 symptomatic toxicities derived from the National Cancer Institute's Common Terminology Criteria for Adverse Events and Karnofsky Performance Status via tablet computers in waiting areas immediately preceding scheduled visits. During visits, clinicians viewed patients' self-reported toxicity and performance status ratings on a computer interface and could agree or disagree/reassign grades ("shared" reporting). Agreement of clinicians with patient-reported grades was tabulated, and compared using weighted kappa statistics. Clinical actions in response to patient-reported severe (grade 3/4) toxicities were measured (e.g. treatment discontinuation, dose reduction, supportive medications). For comparison, 45 non-trial patients with lung cancer being treated in the same clinic by the same physicians were simultaneously enrolled in a parallel cohort study in which patients also self-reported toxicity grades but reports were not shared with clinicians ("non-shared" reporting).
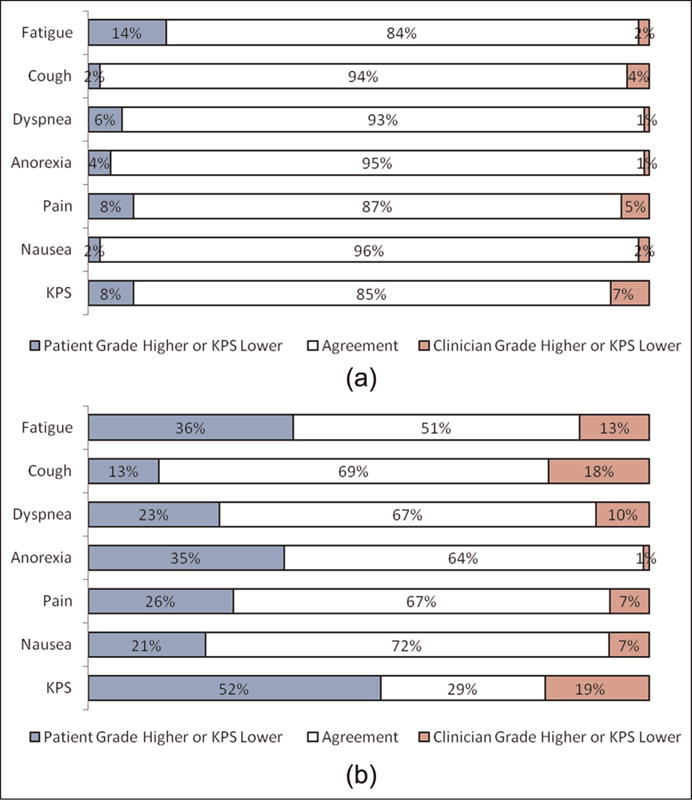
Results: Toxicities and performance status were reported by patients and reviewed by clinicians at (780/782) 99.7% of study visits in the phase 2 trial which used "shared" reporting. Clinicians agreed with patients 93% of the time with kappas 0.82-0.92. Clinical actions were taken in response to 67% of severe patient-reported toxicities. In the "non-shared" reporting comparison group, clinicians agreed with patients 56% of the time with kappas 0.04-0.48 (significantly worse than shared reporting for all symptoms), and clinical actions were taken in response to 44% of severe patient-reported toxicities.
Conclusion: Clinicians will frequently agree with patient-reported symptoms and performance status, and will use this information to guide documentation and symptom management. (ClinicalTrials.gov: NCT00807573).
Keywords: Patient-reported outcome; adverse event; clinical trial; drug development; toxicity.
© The Author(s) 2015.
Conflict of interest statement
Declaration of Conflicting Interests The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Henry DH, Viswanathan HN, Elkin EP, et al. Symptoms and treatment burden associated with cancer treatment: results from a cross-sectional national survey in the U.S. Support Care Cancer. 2008;16:791–801. - PubMed
-
- National Cancer Institute, National Institutes of Health, U.S. Department of Health and Human Services. (NIH publication # 09-7473).Common Terminology Criteria for Adverse Events (CTCAE), version 4.0. Published 29 May 2009; Revised version 4.03 14 June 2010), http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5... (accessed 1 May 2015)
-
- Schag CC, Heinrich RL, Ganz PA. Karnofsky performance status revisited: reliability, validity, and guidelines. J Clin Oncol. 1984;2:187–193. - PubMed
-
- Fromme EK, Eilers KM, Mori M, et al. How accurate is clinician reporting of chemotherapy adverse effects? A comparison with patient-reported symptoms from the Quality-of-Life Questionnaire C30. J Clin Oncol. 2004;22:3485–3490. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
