

Expansion of inflammatory innate lymphoid cells in patients with common variable immune deficiency
- PMID: 26542033
- PMCID: PMC4866594
- DOI: 10.1016/j.jaci.2015.09.013
Expansion of inflammatory innate lymphoid cells in patients with common variable immune deficiency
Abstract
Background: Common variable immunodeficiency (CVID) is an antibody deficiency treated with immunoglobulin; however, patients can have noninfectious inflammatory conditions that lead to heightened morbidity and mortality.
Objectives: Modular analyses of RNA transcripts in whole blood previously identified an upregulation of many interferon-responsive genes. In this study we sought the cell populations leading to this signature.
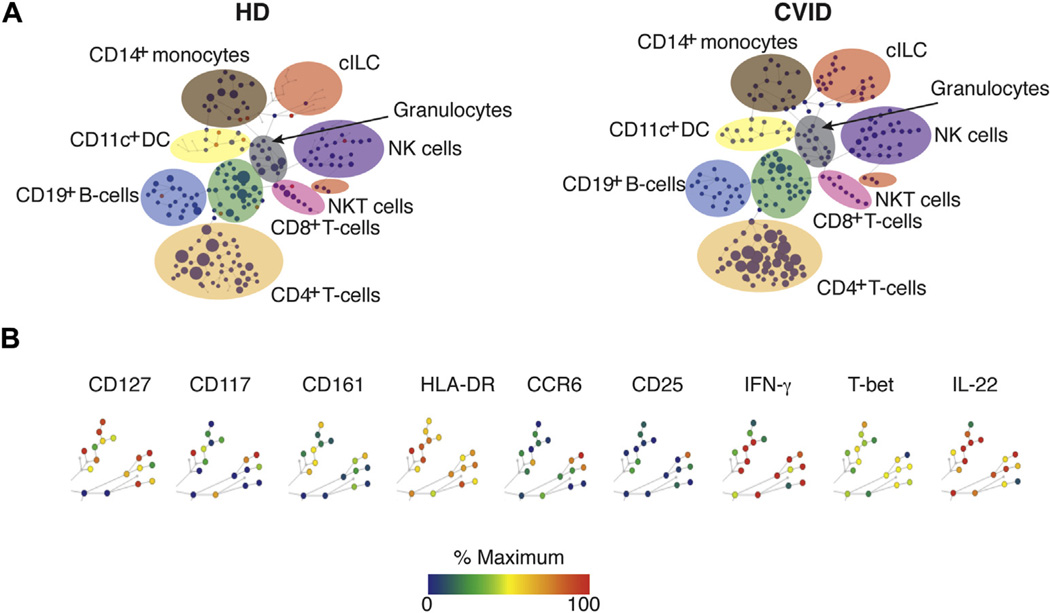
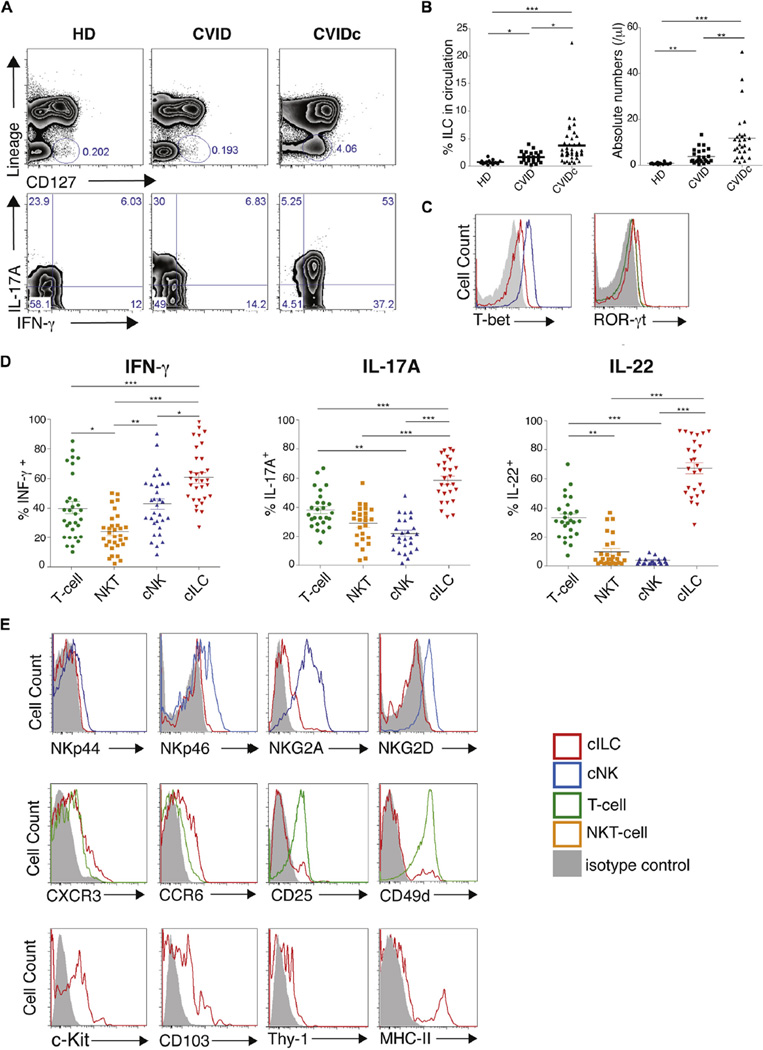
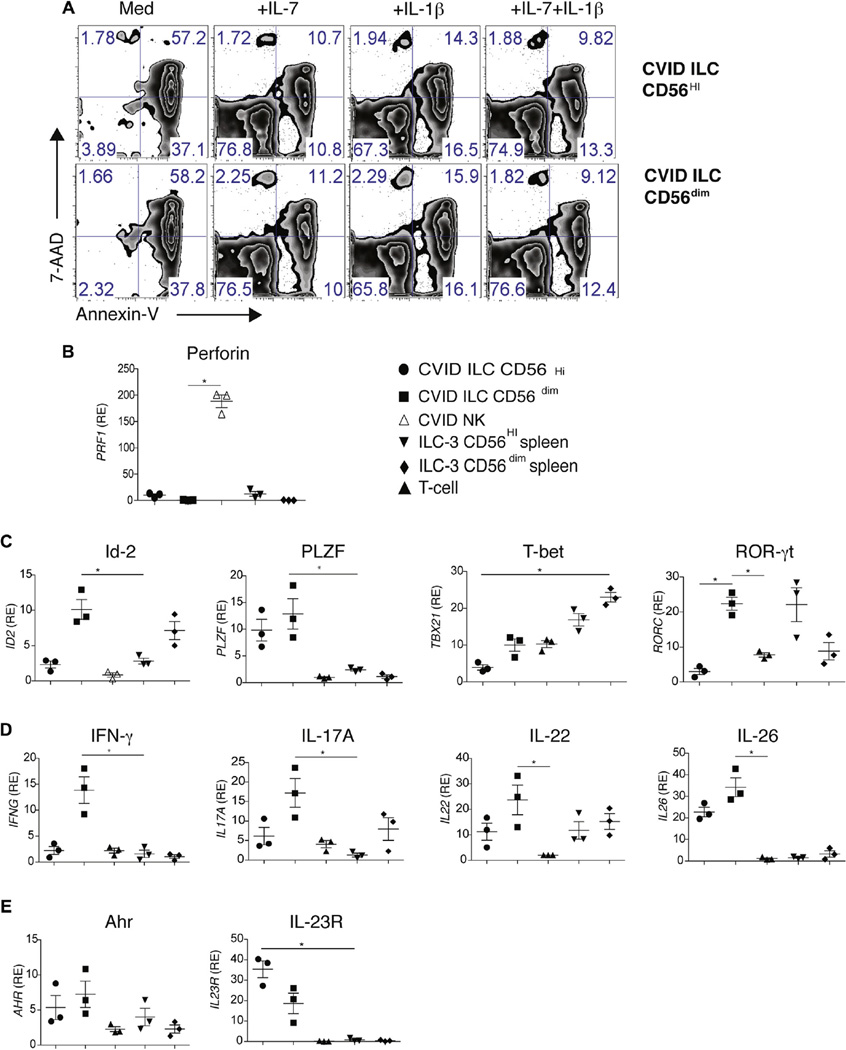
Methods: Lymphoid cells were measured in peripheral blood of 55 patients with CVID (31 with and 24 without inflammatory/autoimmune complications) by using mass cytometry and flow cytometry. Surface markers, cytokines, and transcriptional characteristics of sorted innate lymphoid cells (ILCs) were defined by using quantitative PCR. Gastrointestinal and lung biopsy specimens of subjects with inflammatory disease were stained to seek ILCs in tissues.
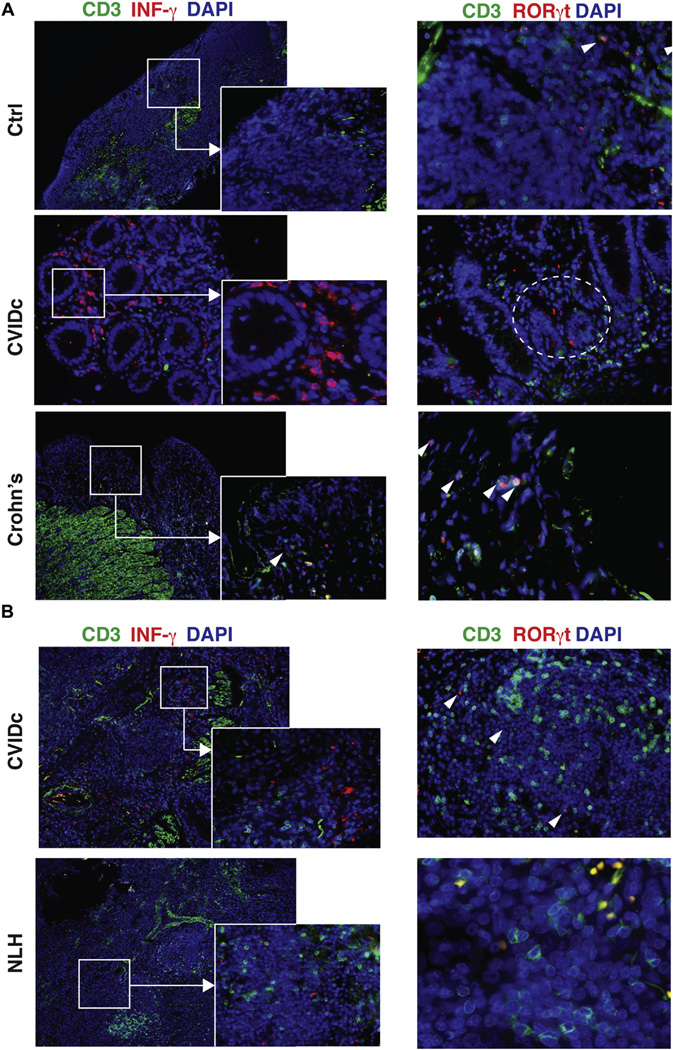
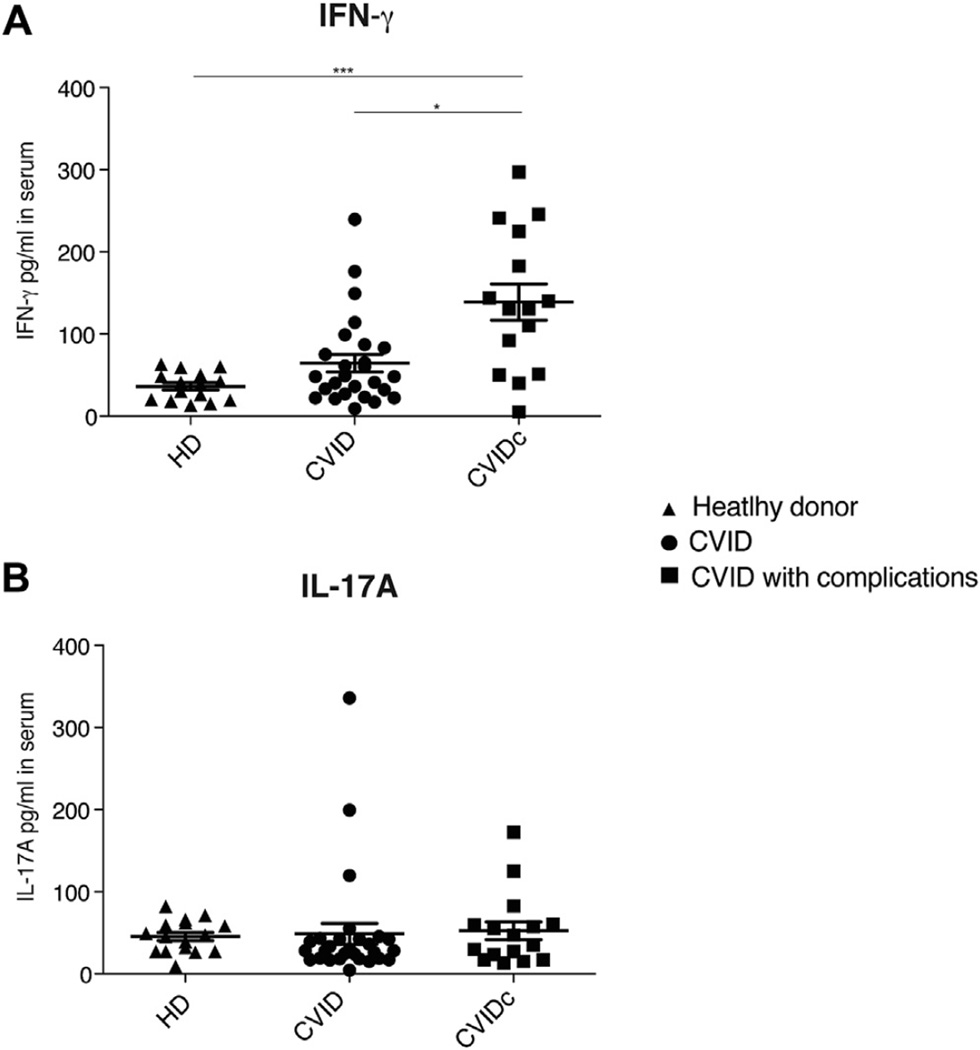
Results: The linage-negative, CD127(+), CD161(+) lymphoid population containing T-box transcription factor, retinoic acid-related orphan receptor (ROR) γt, IFN-γ, IL-17A, and IL-22, all hallmarks of type 3 innate lymphoid cells, were expanded in the blood of patients with CVID with inflammatory conditions (mean, 3.7% of PBMCs). ILCs contained detectable amounts of the transcription factors inhibitor of DNA binding 2, T-box transcription factor, and RORγt and increased mRNA transcripts for IL-23 receptor (IL-23R) and IL-26, demonstrating inflammatory potential. In gastrointestinal and lung biopsy tissues of patients with CVID, numerous IFN-γ(+)RORγt(+)CD3(-) cells were identified, suggesting a role in these mucosal inflammatory states.
Conclusions: An expansion of this highly inflammatory ILC population is a characteristic of patients with CVID with inflammatory disease; ILCs and the interferon signature are markers for the uncontrolled inflammatory state in these patients.
Keywords: Common variable immunodeficiency; inflammatory complications; innate lymphoid cells; mucosal disease.
Copyright © 2015 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure of potential conflict of interest: The rest of the authors declare that they have no relevant conflicts of interest.
Figures
References
-
- Quinti I, Soresina A, Spadaro G, Martino S, Donnanno S, Agostini C, et al. Long-term follow-up and outcome of a large cohort of patients with common variable immunodeficiency. J Clin Immunol. 2007;27:308–316. - PubMed
-
- Wehr C, Kivioja T, Schmitt C, Ferry B, Witte T, Eren E, et al. The EUROclass trial: defining subgroups in common variable immunodeficiency. Blood. 2008;111:77–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
