

Pachychoroid neovasculopathy and age-related macular degeneration
- PMID: 26542071
- PMCID: PMC4635432
- DOI: 10.1038/srep16204
Pachychoroid neovasculopathy and age-related macular degeneration
Abstract
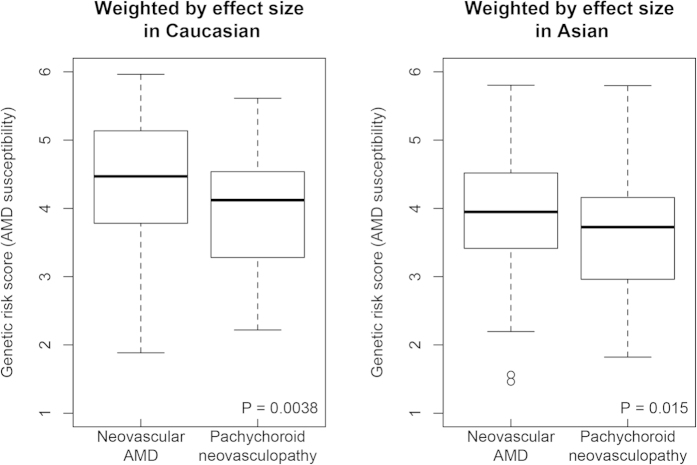
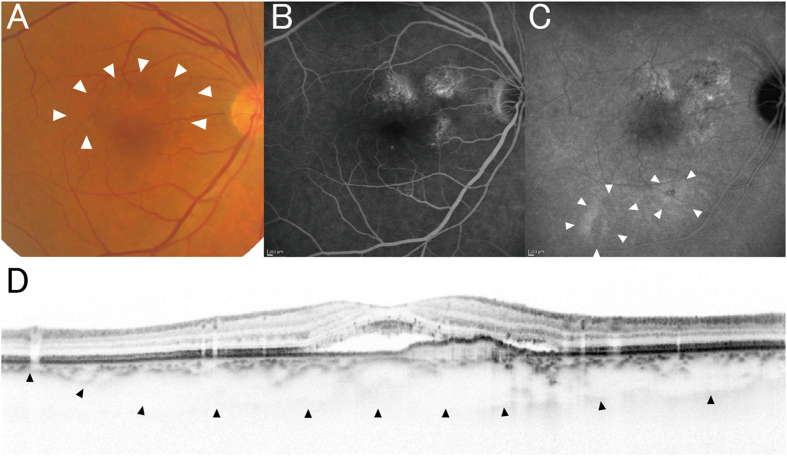
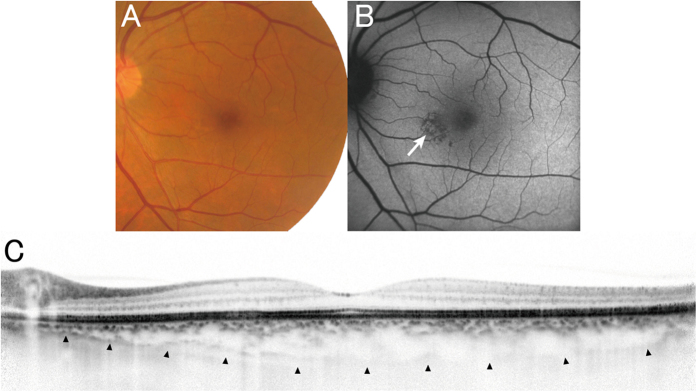
Pachychoroid neovasculopathy is a recently proposed clinical entity of choroidal neovascularization (CNV). As it often masquerades as neovascular age-related macular degeneration (AMD), it is currently controversial whether pachychoroid neovasculopathy should be distinguished from neovascular AMD. This is because its characteristics have yet to be well described. To estimate the relative prevalence of pachychoroid neovasculopathy in comparison with neovascular AMD and to investigate the phenotypic/genetic differences of the two diseases, we evaluated 200 consecutive Japanese patients who agreed to participate in the genetic study and diagnosed with pachychoroid neovasculopathy or neovascular AMD. Pachychoroid neovasculopathy was observed in 39 individuals (19.5%), which corresponds to one fourth of neovascular AMD. Patients with pachychoroid neovasculopathy were significantly younger (p = 5.1 × 10(-5)) and showed a greater subfoveal choroidal thickness (p = 3.4 × 10(-14)). Their genetic susceptibility to AMD was significantly lower than that of neovascular AMD; ARMS2 rs10490924 (p = 0.029), CFH rs800292 (p = 0.013) and genetic risk score calculated from 11 AMD susceptibility genes (p = 3.8 × 10(-3)). Current results implicate that the etiologies of the two conditions must be different. Thus, it will be necessary to distinguish these two conditions in future studies.
Figures
References
-
- Kawasaki R. et al. Prevalence and risk factors for age-related macular degeneration in an adult Japanese population: the Funagata study. Ophthalmology 115, 1376–81, 1381 e1-2 (2008). - PubMed
-
- Kawasaki R. et al. The prevalence of age-related macular degeneration in Asians: a systematic review and meta-analysis. Ophthalmology 117, 921–7 (2010). - PubMed
-
- Varma R., Fraser-Bell S., Tan S., Klein R. & Azen S. P. Prevalence of age-related macular degeneration in Latinos: the Los Angeles Latino eye study. Ophthalmology 111, 1288–97 (2004). - PubMed
-
- Edwards A. O. et al. Complement factor H polymorphism and age-related macular degeneration. Science 308, 421–4 (2005). - PubMed
-
- Haines J. L. et al. Complement factor H variant increases the risk of age-related macular degeneration. Science 308, 419–21 (2005). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
