

Proximal segmentation of the dorsal mesogastrium reveals new anatomical implications for laparoscopic surgery
- PMID: 26542081
- PMCID: PMC4635343
- DOI: 10.1038/srep16287
Proximal segmentation of the dorsal mesogastrium reveals new anatomical implications for laparoscopic surgery
Abstract
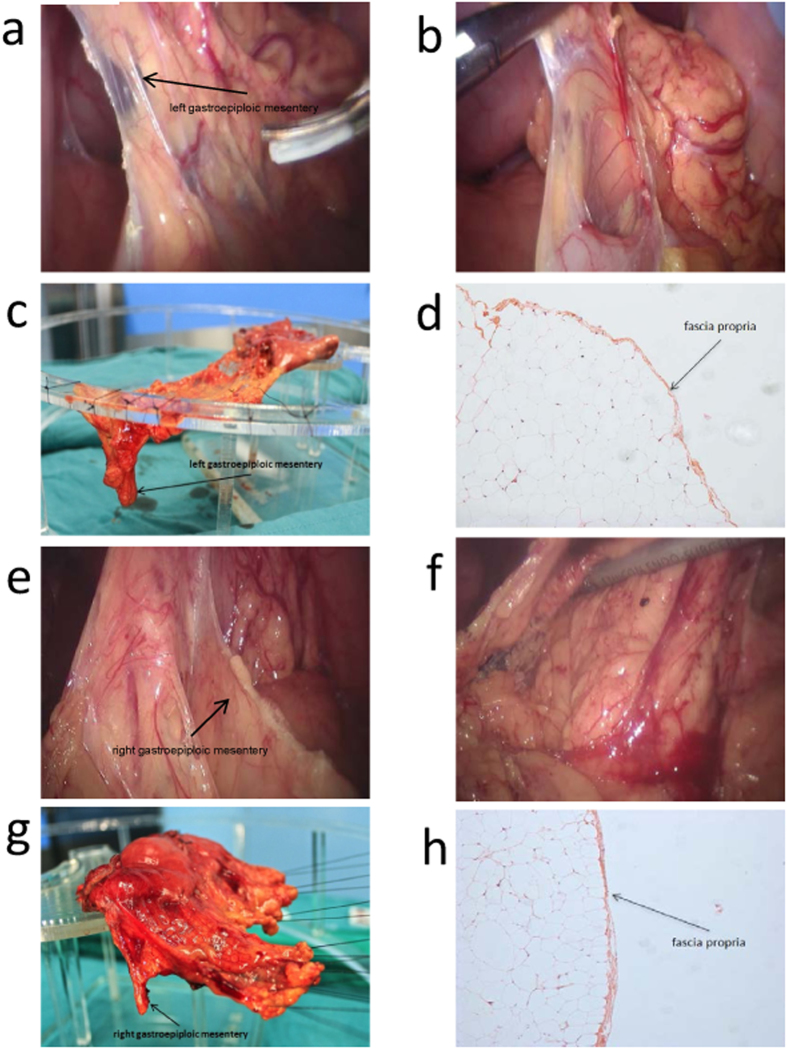
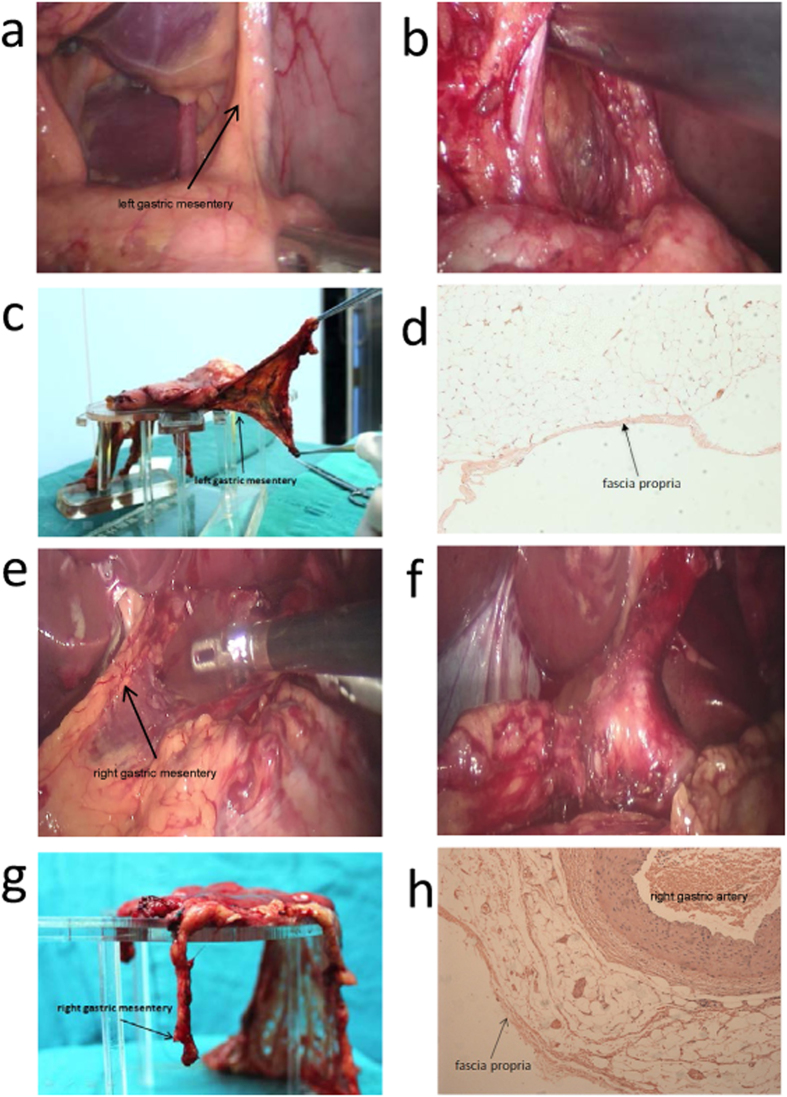
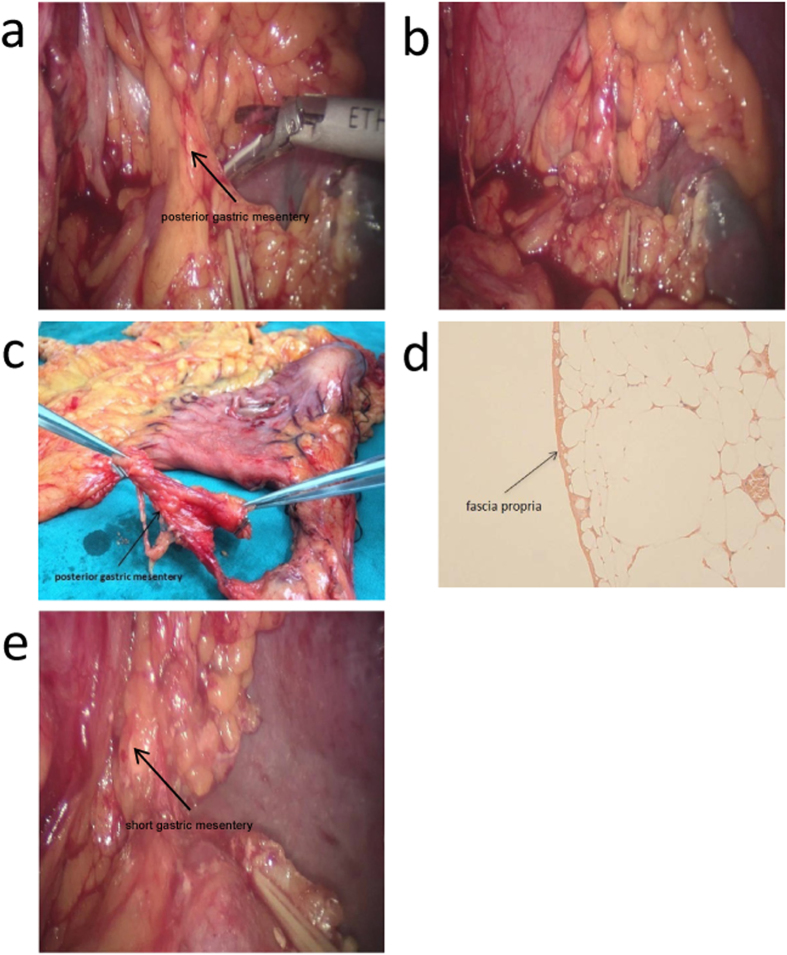
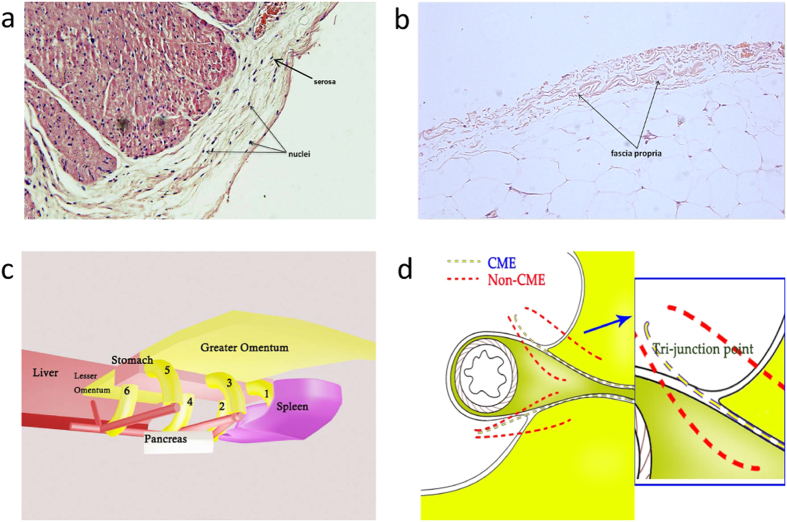
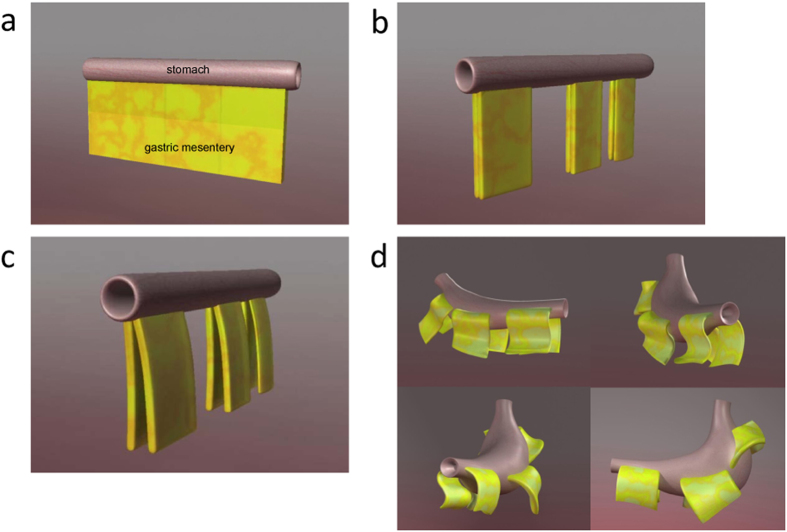
Generally, the gold standard of radical surgery for gastrointestinal (GI) tumors is en bloc resection of primary lesions and their related tissues. For gastric cancer, the ideal surgical treatment should be D2 radical gastrectomy plus complete mesogastrium excision. Complete mesogastrium excision is rarely done or mentioned since little is known about the mesogastrium and its presence is still with controversy. Topographically, the "mesogastrium" refers to a peri-gastric structure composed of "fascia propria", enveloping lymph nodes, blood vessels and adipose tissues, which by connecting to the stomach, suspends from the posterior abdominal wall. In this study, by employing video laparoscopy, a number of proximal segments of dorsal mesogastrium were found being extensively scattered around the pancreas. The structure of the mesogastrium was further identified intraoperatively and then confirmed both grossly and histologically after the operation. Our results demonstrated the existence of mesogastrium (gastric mesentery) and its architecture. We suggest for the first time a "Table model" to describe the relationship between the stomach and gastric mesenteries enveloped by fascia propria, which might provide an improvement in the surgical methods for excision of gastric cancer.
Figures
References
-
- Davydov M. I. New surgical technologies in oncology. Vestn Ross Akad Med Nauk 10, 4–9 (2007). - PubMed
-
- Enker W. E., Thaler H. T., Cranor M. L. & Polyak T. Total mesorectal excision in the operative treatment of carcinoma of the rectum. J Am Coll Surg 181, 335–346 (1995). - PubMed
-
- Carlsen E., Schlichting E., Guldvog I., Johnson E. & Heald R. J. Effect of the introduction of total mesorectal excision for the treatment of rectal cancer. The British journal of surgery 85, 526–529 (1998). - PubMed
-
- Peeters K. C. et al. The TME trial after a median follow-up of 6 years: increased local control but no survival benefit in irradiated patients with resectable rectal carcinoma. Ann Surg 246, 693–701 (2007). - PubMed
-
- West N. P. et al. Complete mesocolic excision with central vascular ligation produces an oncologically superior specimen compared with standard surgery for carcinoma of the colon. J Clin Oncol 28, 272–278 (2010). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
