

A phase 1 clinical trial of the selective BTK inhibitor ONO/GS-4059 in relapsed and refractory mature B-cell malignancies
- PMID: 26542378
- PMCID: PMC4731845
- DOI: 10.1182/blood-2015-08-664086
A phase 1 clinical trial of the selective BTK inhibitor ONO/GS-4059 in relapsed and refractory mature B-cell malignancies
Abstract
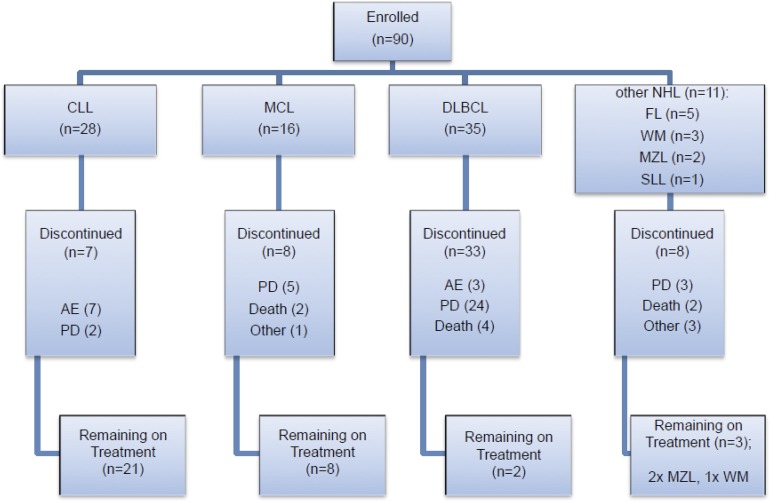
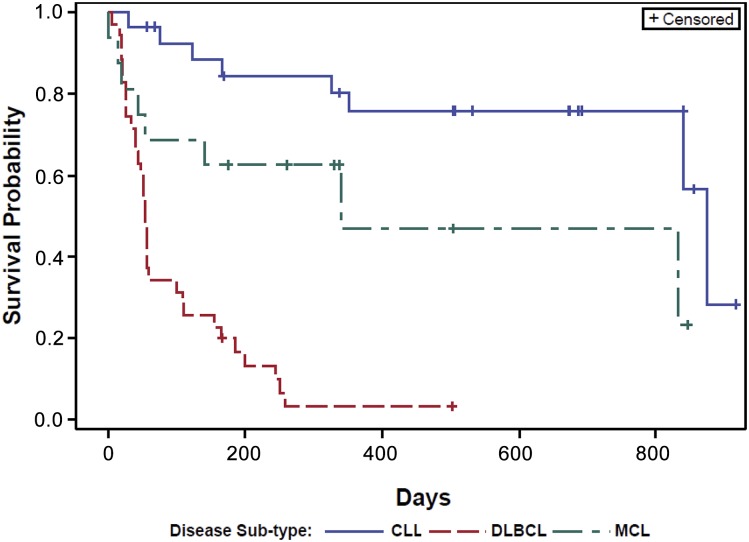
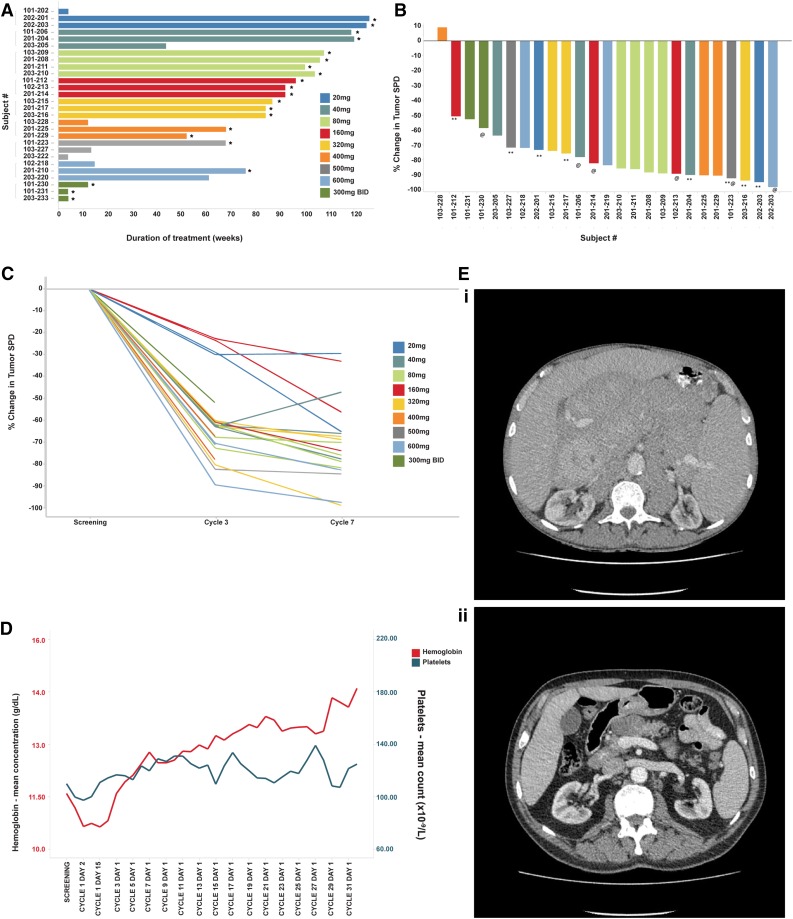
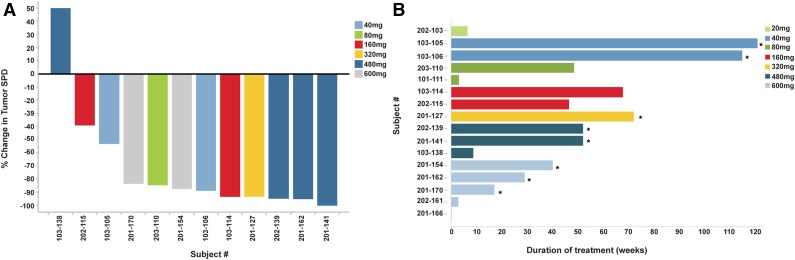
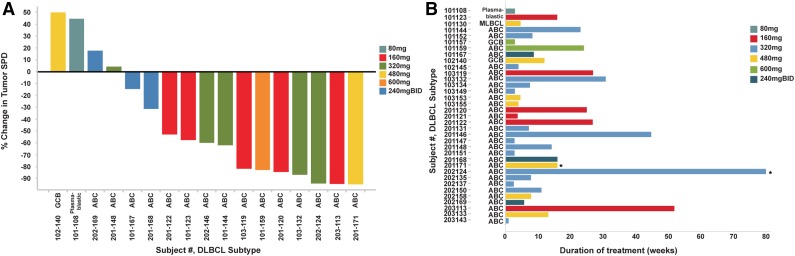
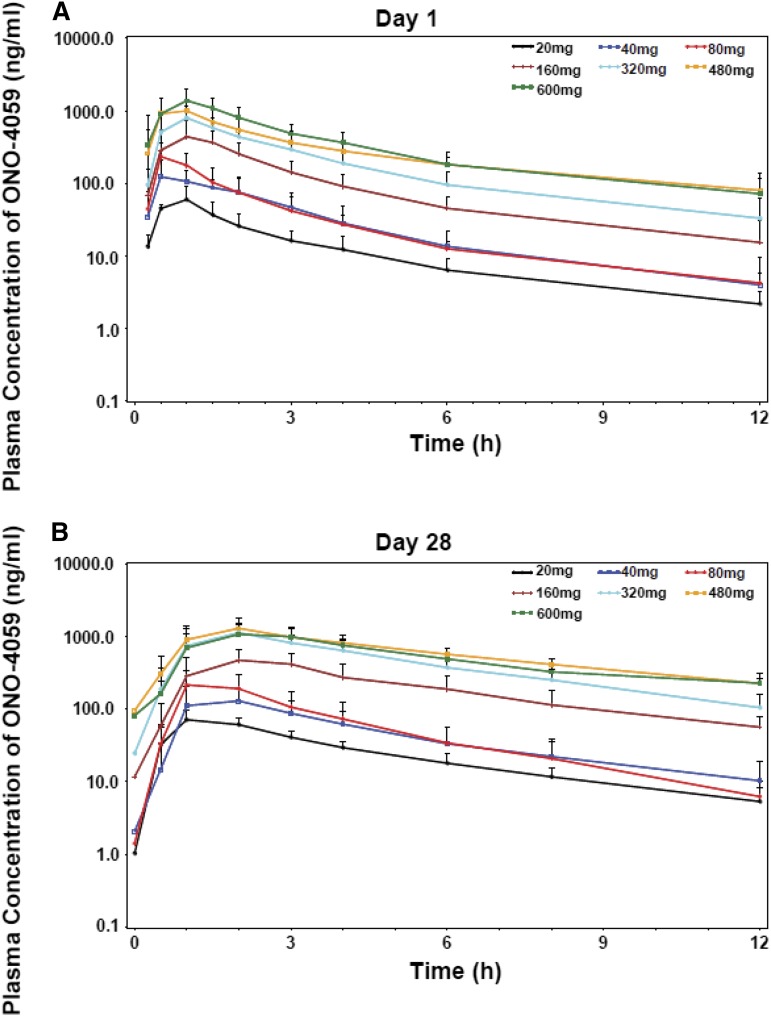
We report the results of a multicenter phase 1 dose-escalation study of the selective Bruton tyrosine kinase (BTK) inhibitor ONO/GS-4059 in 90 patients with relapsed/refractory B-cell malignancies. There were 9 dose-escalation cohorts ranging from 20 mg to 600 mg once daily with twice-daily regimens of 240 mg and 300 mg. Twenty-four of 25 evaluable chronic lymphocytic leukemia (CLL) patients (96%) responded to ONO/GS-4059, with a median treatment duration of 80 weeks; 21 CLL patients remain on treatment. Lymph node responses were rapid and associated with a concurrent lymphocytosis. Eleven of 12 evaluable patients with mantle cell lymphoma (92%) responded (median treatment duration, 40 weeks). Eleven of 31 non-germinal center B-cell diffuse large B-cell lymphoma patients (35%) responded but median treatment duration was 12 weeks due to development of progressive disease. ONO/GS-4059 was very well tolerated with 75% of adverse events (AEs) being Common Toxicity Criteria for Adverse Events version 4.0 grade 1 or grade 2. Grade 3/4 AEs were mainly hematologic and recovered spontaneously during therapy. One CLL patient experienced a grade 3 treatment-related bleeding event (spontaneous muscle hematoma) but no clinically significant diarrhea, cardiac dysrhythmias, or arthralgia were observed. No maximal tolerated dose (MTD) was reached in the CLL cohort. In the non-Hodgkin lymphoma cohort, 4 patients developed a dose-limiting toxicity, yielding an MTD of 480 mg once daily. ONO/GS-4059 has significant activity in relapsed/refractory B-cell malignancies without major drug-related toxicity. The selectivity of ONO/GS-4059 should confer advantages in combination therapies. This trial was registered at www.clinicaltrials.gov as #NCT01659255.
© 2016 by The American Society of Hematology.
Figures
References
-
- Mohamed AJ, Yu L, Bäckesjö CM, et al. Bruton’s tyrosine kinase (Btk): function, regulation, and transformation with special emphasis on the PH domain. Immunol Rev. 2009;228(1):58–73. - PubMed
-
- de Weers M, Verschuren MC, Kraakman ME, et al. The Bruton’s tyrosine kinase gene is expressed throughout B cell differentiation, from early precursor B cell stages preceding immunoglobulin gene rearrangement up to mature B cell stages. Eur J Immunol. 1993;23(12):3109–3114. - PubMed
-
- Saito K, Scharenberg AM, Kinet JP. Interaction between the Btk PH domain and phosphatidylinositol-3,4,5-trisphosphate directly regulates Btk. J Biol Chem. 2001;276(19):16201–16206. - PubMed
-
- Hendriks RW, Bredius RG, Pike-Overzet K, Staal FJ. Biology and novel treatment options for XLA, the most common monogenetic immunodeficiency in man. Expert Opin Ther Targets. 2011;15(8):1003–1021. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
