

Time trends in coronary revascularization procedures among people with COPD: analysis of the Spanish national hospital discharge data (2001-2011)
- PMID: 26543361
- PMCID: PMC4622492
- DOI: 10.2147/COPD.S92614
Time trends in coronary revascularization procedures among people with COPD: analysis of the Spanish national hospital discharge data (2001-2011)
Abstract
Background: People with COPD suffering from coronary artery disease are frequently treated with revascularization procedures. We aim to compare trends in the use and outcomes of these procedures in COPD and non-COPD patients in Spain between 2001 and 2011.
Methods: We identified all patients who had undergone percutaneous coronary interventions (PCIs) and coronary artery bypass graft (CABG) surgeries, using national hospital discharge data. Discharges were grouped into: COPD and no COPD.
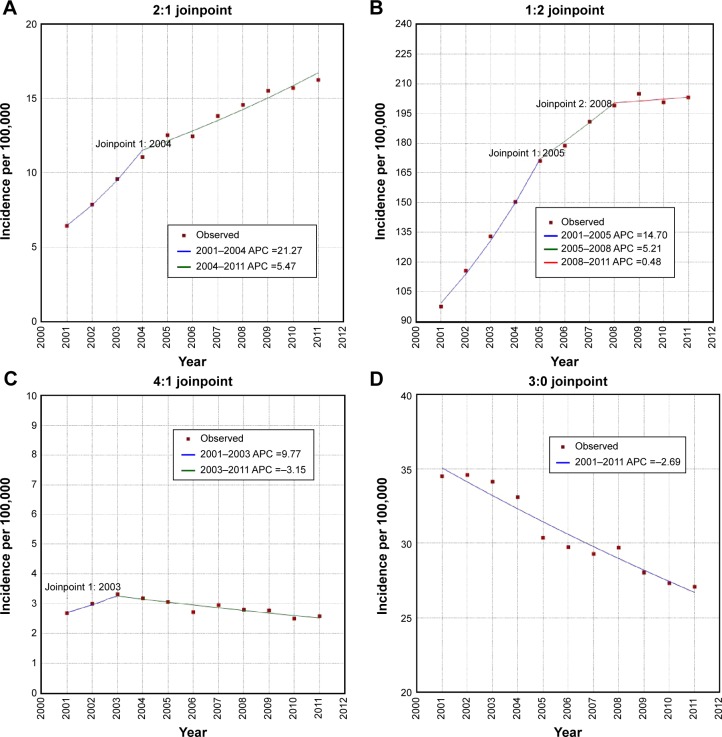
Results: From 2001 to 2011, 428,516 PCIs and 79,619 CABGs were performed. The sex and age-adjusted use of PCI increased by 21.27% per year from 2001 to 2004 and by 5.47% per year from 2004 to 2011 in patients with COPD. In-hospital mortality (IHM) among patients with COPD who underwent a PCI increased significantly from 2001 to 2011 (odds ratio 1.11; 95% confidence interval 1.03-1.20). Among patients with COPD who underwent a CABG, the sex and age-adjusted CABG incidence rate increased by 9.77% per year from 2001 to 2003, and then decreased by 3.15% through 2011. The probability of dying during hospitalization in patients who underwent a CABG did not change significantly in patients with and without COPD (odds ratio, 1.06; 95% confidence interval 0.96-1.17).
Conclusion: The annual percent change in PCI procedures increased in COPD and non-COPD patients. We found a decrease in the use of CABG procedures in both groups. IHM was higher in patients with COPD who underwent a PCI than in those without COPD. However, COPD did not increase the probability of dying during hospitalization in patients who underwent a CABG.
Keywords: COPD; coronary artery bypass graft surgery; hospitalization; in-hospital mortality; length of stay; percutaneous coronary intervention.
Figures
Similar articles
-
National trends in utilization and outcomes of coronary revascularization procedures among people with and without type 2 diabetes in Spain (2001-2011).Cardiovasc Diabetol. 2014 Jan 3;13:3. doi: 10.1186/1475-2840-13-3. Cardiovasc Diabetol. 2014. PMID: 24383412 Free PMC article.
-
Outcome of patients with chronic obstructive pulmonary disease and severe coronary artery disease who had a coronary artery bypass graft or a percutaneous coronary intervention.Eur J Cardiothorac Surg. 2017 Nov 1;52(5):930-936. doi: 10.1093/ejcts/ezx219. Eur J Cardiothorac Surg. 2017. PMID: 29088423
-
Changes in the Practice of Coronary Revascularization between 2006 and 2010 in the Republic of Korea.Yonsei Med J. 2015 Jul;56(4):895-903. doi: 10.3349/ymj.2015.56.4.895. Yonsei Med J. 2015. PMID: 26069109 Free PMC article.
-
Survival in patients with peripheral vascular disease after percutaneous coronary intervention and coronary artery bypass graft surgery.Ann Thorac Surg. 2004 Aug;78(2):466-70; discussion 470. doi: 10.1016/j.athoracsur.2004.01.044. Ann Thorac Surg. 2004. PMID: 15276497 Review.
-
Isolated disease of the proximal left anterior descending artery comparing the effectiveness of percutaneous coronary interventions and coronary artery bypass surgery.JACC Cardiovasc Interv. 2008 Oct;1(5):483-91. doi: 10.1016/j.jcin.2008.07.001. JACC Cardiovasc Interv. 2008. PMID: 19463349 Review.
Cited by
-
Global Insights into Chronic Obstructive Pulmonary Disease and Coronary Artery Disease: A Systematic Review and Meta-Analysis of 6,400,000 Patients.Rev Cardiovasc Med. 2024 Jan 15;25(1):25. doi: 10.31083/j.rcm2501025. eCollection 2024 Jan. Rev Cardiovasc Med. 2024. PMID: 39077650 Free PMC article.
-
Coronary endarterectomy: an old tool for patients currently operated on with coronary artery bypass grafting. Long-term results, risk factor analysis.Kardiochir Torakochirurgia Pol. 2018 Dec;15(4):219-226. doi: 10.5114/kitp.2018.80917. Epub 2018 Dec 31. Kardiochir Torakochirurgia Pol. 2018. PMID: 30647744 Free PMC article.
-
Chronic obstructive pulmonary disease and periprocedural complications in patients undergoing percutaneous coronary interventions.PLoS One. 2018 Oct 1;13(10):e0204257. doi: 10.1371/journal.pone.0204257. eCollection 2018. PLoS One. 2018. PMID: 30273363 Free PMC article.
-
Trends in Utilization and In-hospital Outcomes of Cardiac Surgery.Braz J Cardiovasc Surg. 2020 Apr 1;35(2):VII-IX. doi: 10.21470/1678-9741-1-2020-0603. Braz J Cardiovasc Surg. 2020. PMID: 32369289 Free PMC article. No abstract available.
References
-
- Friedman GD, Klatsky AL, Siegelaub AB. Lung function and risk of myocardial infarction and sudden cardiac death. N Engl J Med. 1976;294(20):1071–1075. - PubMed
-
- Sidney S, Sorel M, Quesenberry CP, Jr, DeLuise C, Lanes S, Eisner MD. COPD and incident cardiovascular disease hospitalizations and mortality: Kaiser Permanente Medical Care Program. Chest. 2005;128(4):2068–2075. - PubMed
-
- Young RP, Hopkins R, Eaton TE. Forced expiratory volume in one second: not just a lung function test but a marker of premature death from all causes. Eur Respir J. 2007;30(4):616–622. - PubMed
-
- Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. - PubMed
-
- Konecny T, Somers K, Orban M, et al. Interactions between COPD and outcomes after percutaneous coronary intervention. Chest. 2010;138(3):621–627. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
