

Effect of Financial Incentives to Physicians, Patients, or Both on Lipid Levels: A Randomized Clinical Trial
- PMID: 26547464
- PMCID: PMC5509443
- DOI: 10.1001/jama.2015.14850
Effect of Financial Incentives to Physicians, Patients, or Both on Lipid Levels: A Randomized Clinical Trial
Abstract
Importance: Financial incentives to physicians or patients are increasingly used, but their effectiveness is not well established.
Objective: To determine whether physician financial incentives, patient incentives, or shared physician and patient incentives are more effective than control in reducing levels of low-density lipoprotein cholesterol (LDL-C) among patients with high cardiovascular risk.
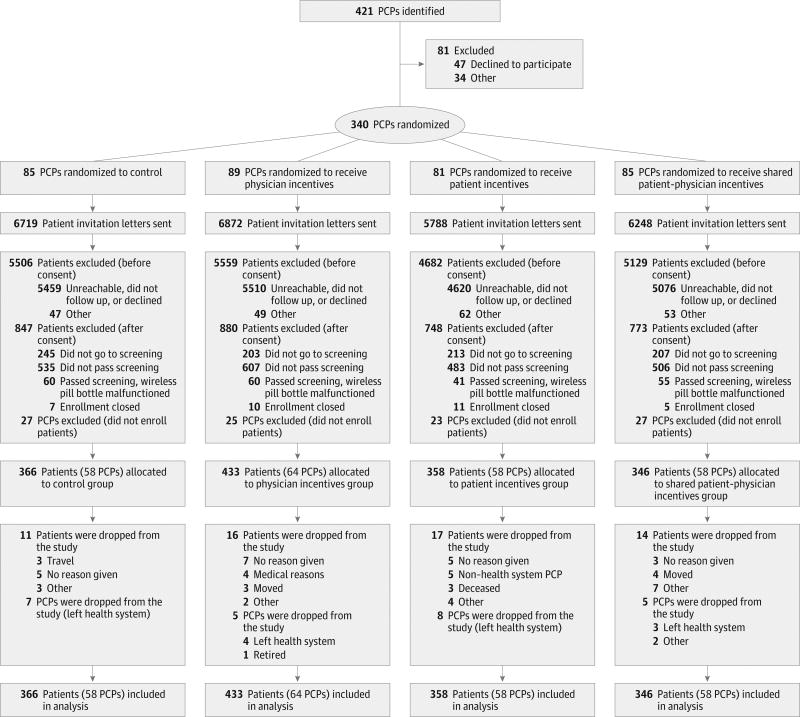
Design, setting, and participants: Four-group, multicenter, cluster randomized clinical trial with a 12-month intervention conducted from 2011 to 2014 in 3 primary care practices in the northeastern United States. Three hundred forty eligible primary care physicians (PCPs) were enrolled from a pool of 421. Of 25,627 potentially eligible patients of those PCPs, 1503 enrolled. Patients aged 18 to 80 years were eligible if they had a 10-year Framingham Risk Score (FRS) of 20% or greater, had coronary artery disease equivalents with LDL-C levels of 120 mg/dL or greater, or had an FRS of 10% to 20% with LDL-C levels of 140 mg/dL or greater. Investigators were blinded to study group, but participants were not.
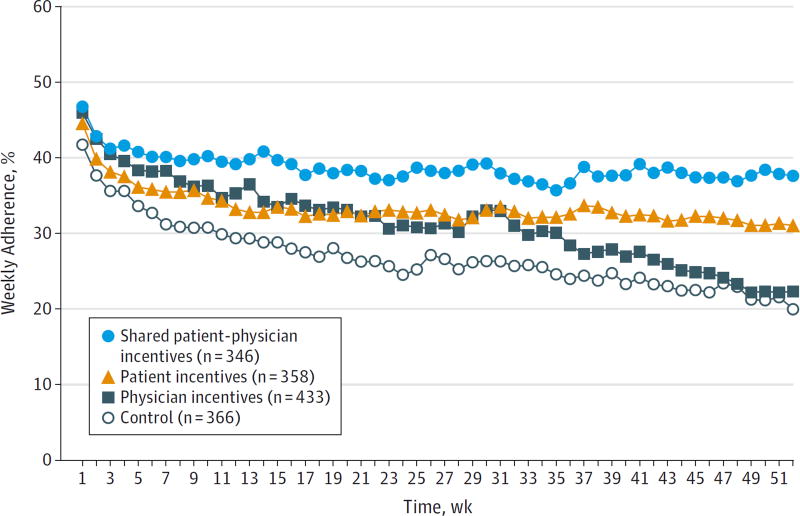
Interventions: Primary care physicians were randomly assigned to control, physician incentives, patient incentives, or shared physician-patient incentives. Physicians in the physician incentives group were eligible to receive up to $1024 per enrolled patient meeting LDL-C goals. Patients in the patient incentives group were eligible for the same amount, distributed through daily lotteries tied to medication adherence. Physicians and patients in the shared incentives group shared these incentives. Physicians and patients in the control group received no incentives tied to outcomes, but all patient participants received up to $355 each for trial participation.
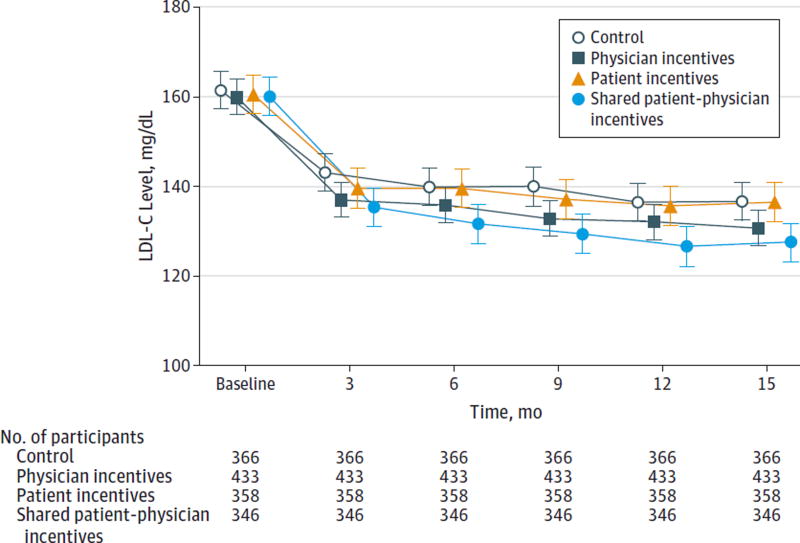
Main outcomes and measures: Change in LDL-C level at 12 months.
Results: Patients in the shared physician-patient incentives group achieved a mean reduction in LDL-C of 33.6 mg/dL (95% CI, 30.1-37.1; baseline, 160.1 mg/dL; 12 months, 126.4 mg/dL); those in physician incentives achieved a mean reduction of 27.9 mg/dL (95% CI, 24.9-31.0; baseline, 159.9 mg/dL; 12 months, 132.0 mg/dL); those in patient incentives achieved a mean reduction of 25.1 mg/dL (95% CI, 21.6-28.5; baseline, 160.6 mg/dL; 12 months, 135.5 mg/dL); and those in the control group achieved a mean reduction of 25.1 mg/dL (95% CI, 21.7-28.5; baseline, 161.5 mg/dL; 12 months, 136.4 mg/dL; P < .001 for comparison of all 4 groups). Only patients in the shared physician-patient incentives group achieved reductions in LDL-C levels statistically different from those in the control group (8.5 mg/dL; 95% CI, 3.8-13.3; P = .002).
Conclusions and relevance: In primary care practices, shared financial incentives for physicians and patients, but not incentives to physicians or patients alone, resulted in a statistically significant difference in reduction of LDL-C levels at 12 months. This reduction was modest, however, and further information is needed to understand whether this approach represents good value.
Trial registration: clinicaltrials.gov Identifier: NCT01346189.
Conflict of interest statement
Figures
Comment in
-
Multiple Imputation: A Flexible Tool for Handling Missing Data.JAMA. 2015 Nov 10;314(18):1966-7. doi: 10.1001/jama.2015.15281. JAMA. 2015. PMID: 26547468 Free PMC article. No abstract available.
-
[Effect of financial incentives on LDL-cholesterol levels].Semergen. 2016 Nov-Dec;42(8):e144-e145. doi: 10.1016/j.semerg.2015.12.008. Epub 2016 Feb 6. Semergen. 2016. PMID: 26860880 Spanish. No abstract available.
-
Financial Incentives and Cholesterol Levels.JAMA. 2016 Apr 19;315(15):1657-8. doi: 10.1001/jama.2016.0309. JAMA. 2016. PMID: 27092834 No abstract available.
-
Financial Incentives and Cholesterol Levels--Reply.JAMA. 2016 Apr 19;315(15):1658. doi: 10.1001/jama.2016.0315. JAMA. 2016. PMID: 27092836 No abstract available.
References
-
- Baigent C, Keech A, Kearney PM, et al. Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366(9493):1267–1278. - PubMed
-
- Austin PC, Mamdani MM, Juurlink DN, Alter DA, Tu JV. Missed opportunities in the secondary prevention of myocardial infarction: an assessment of the effects of statin underprescribing on mortality. Am Heart J. 2006;151(5):969–975. - PubMed
-
- Albert NM, Birtcher KK, Cannon CP, et al. Factors associated with discharge lipid-lowering drug prescription in patients hospitalized for coronary artery disease (from the Get With the Guidelines database) Am J Cardiol. 2008;101(9):1242–1246. - PubMed
-
- Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA. 2002;288(4):462–467. - PubMed
-
- Ho PM, Spertus JA, Masoudi FA, et al. Impact of medication therapy discontinuation on mortality after myocardial infarction. Arch Intern Med. 2006;166(17):1842–1847. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
