

Cancer immunotherapy: Strategies for personalization and combinatorial approaches
- PMID: 26548534
- PMCID: PMC4684975
- DOI: 10.1016/j.molonc.2015.10.009
Cancer immunotherapy: Strategies for personalization and combinatorial approaches
Abstract
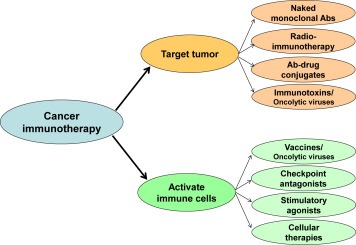
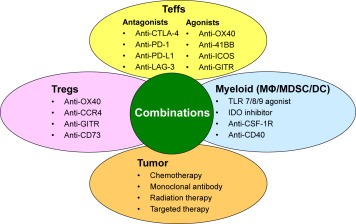
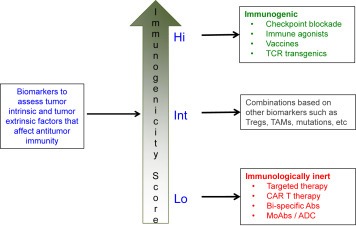
The results of recent clinical trials using novel immunotherapy strategies such as immune checkpoint blockade and adoptive T-cell therapy approaches including CAR T-cell therapy have clearly established immunotherapy as an important modality for the treatment of cancer besides the traditional approaches of surgery, radiotherapy, and chemotherapy or targeted therapy. However, to date immunotherapy has been shown to induce durable clinical benefit in only a fraction of the patients. The use of combination strategies is likely to increase the number of patients that might benefit from immunotherapy. Indeed, over the last decade, the characterization of multiple immune resistance mechanisms used by the tumor to evade the immune system and the development of agents that target those mechanisms has generated a lot of enthusiasm for cancer immunotherapy. But a critical issue is to determine how best to combine such agents. This review will focus on novel immunotherapy agents currently in development and discuss strategies to develop and personalize combination cancer immunotherapy strategies.
Keywords: Cancer; Immune checkpoint; Immunotherapy; Personalized; T cells.
Copyright © 2015 Federation of European Biochemical Societies. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Angell, H. , Galon, J. , 2013. From the immune contexture to the immunoscore: the role of prognostic and predictive immune markers in cancer. Curr. Opin. Immunol. 25, 261–267. - PubMed
-
- Ansell, S.M. , Lesokhin, A.M. , Borrello, I. , Halwani, A. , Scott, E.C. , Gutierrez, M. , Schuster, S.J. , Millenson, M.M. , Cattry, D. , Freeman, G.J. , Rodig, S.J. , Chapuy, B. , Ligon, A.H. , Zhu, L. , Grosso, J.F. , Kim, S.Y. , Timmerman, J.M. , Shipp, M.A. , Armand, P. , 2015. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin's lymphoma. New Engl. J. Med. 372, 311–319. - PMC - PubMed
-
- Biswas, S.K. , Mantovani, A. , 2010. Macrophage plasticity and interaction with lymphocyte subsets: cancer as a paradigm. Nat. Immunol. 11, 889–896. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
