

Two-Year Outcomes of Surgical Treatment of Severe Ischemic Mitral Regurgitation
- PMID: 26550689
- PMCID: PMC4908819
- DOI: 10.1056/NEJMoa1512913
Two-Year Outcomes of Surgical Treatment of Severe Ischemic Mitral Regurgitation
Abstract
Background: In a randomized trial comparing mitral-valve repair with mitral-valve replacement in patients with severe ischemic mitral regurgitation, we found no significant difference in the left ventricular end-systolic volume index (LVESVI), survival, or adverse events at 1 year after surgery. However, patients in the repair group had significantly more recurrences of moderate or severe mitral regurgitation. We now report the 2-year outcomes of this trial.
Methods: We randomly assigned 251 patients to mitral-valve repair or replacement. Patients were followed for 2 years, and clinical and echocardiographic outcomes were assessed.
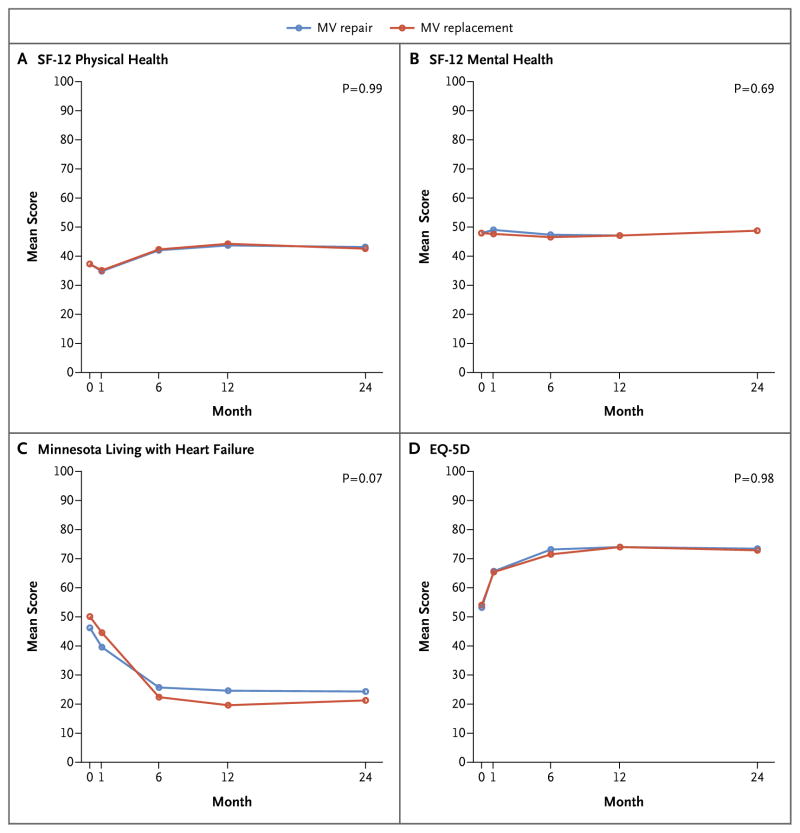
Results: Among surviving patients, the mean (±SD) 2-year LVESVI was 52.6±27.7 ml per square meter of body-surface area with mitral-valve repair and 60.6±39.0 ml per square meter with mitral-valve replacement (mean changes from baseline, -9.0 ml per square meter and -6.5 ml per square meter, respectively). Two-year mortality was 19.0% in the repair group and 23.2% in the replacement group (hazard ratio in the repair group, 0.79; 95% confidence interval, 0.46 to 1.35; P=0.39). The rank-based assessment of LVESVI at 2 years (incorporating deaths) showed no significant between-group difference (z score=-1.32, P=0.19). The rate of recurrence of moderate or severe mitral regurgitation over 2 years was higher in the repair group than in the replacement group (58.8% vs. 3.8%, P<0.001). There were no significant between-group differences in rates of serious adverse events and overall readmissions, but patients in the repair group had more serious adverse events related to heart failure (P=0.05) and cardiovascular readmissions (P=0.01). On the Minnesota Living with Heart Failure questionnaire, there was a trend toward greater improvement in the replacement group (P=0.07).
Conclusions: In patients undergoing mitral-valve repair or replacement for severe ischemic mitral regurgitation, we observed no significant between-group difference in left ventricular reverse remodeling or survival at 2 years. Mitral regurgitation recurred more frequently in the repair group, resulting in more heart-failure-related adverse events and cardiovascular admissions. (Funded by the National Institutes of Health and Canadian Institutes of Health Research; ClinicalTrials.gov number, NCT00807040.).
Figures



Comment in
-
Valvular disease: Functional mitral regurgitation: should all valves be replaced?Nat Rev Cardiol. 2016 Feb;13(2):65-6. doi: 10.1038/nrcardio.2015.206. Epub 2016 Jan 4. Nat Rev Cardiol. 2016. PMID: 26727300 No abstract available.
-
Surgery for Severe Ischemic Mitral Regurgitation.N Engl J Med. 2016 May 19;374(20):1992-3. doi: 10.1056/NEJMc1602607. N Engl J Med. 2016. PMID: 27192684 No abstract available.
-
Surgery for Severe Ischemic Mitral Regurgitation.N Engl J Med. 2016 May 19;374(20):1992. doi: 10.1056/NEJMc1602607. N Engl J Med. 2016. PMID: 27192685 No abstract available.
-
Surgery for Severe Ischemic Mitral Regurgitation.N Engl J Med. 2016 May 19;374(20):1992. doi: 10.1056/NEJMc1602607. N Engl J Med. 2016. PMID: 27192686 No abstract available.
References
-
- Lamas GA, Mitchell GF, Flaker GC, et al. Clinical significance of mitral regurgitation after acute myocardial infarction. Circulation. 1997;96:827–33. - PubMed
-
- Hickey MS, Smith LR, Muhlbaier LH, et al. Current prognosis of ischemic mitral regurgitation. Implications for future management. Circulation. 1988;78:I51–9. - PubMed
-
- Rossi A, Dini FL, Faggiano P, et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure: a quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy. Heart. 2011;97:1675–80. - PubMed
-
- Bonow RO, Carabello BA, Kanu C, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. Circulation. 2006;114(5):e84–231. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical