

A Randomized Trial of Intensive versus Standard Blood-Pressure Control
- PMID: 26551272
- PMCID: PMC4689591
- DOI: 10.1056/NEJMoa1511939
A Randomized Trial of Intensive versus Standard Blood-Pressure Control
Erratum in
-
A Randomized Trial of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2017 Dec 21;377(25):2506. doi: 10.1056/NEJMx170008. N Engl J Med. 2017. PMID: 29262284 No abstract available.
Abstract
Background: The most appropriate targets for systolic blood pressure to reduce cardiovascular morbidity and mortality among persons without diabetes remain uncertain.
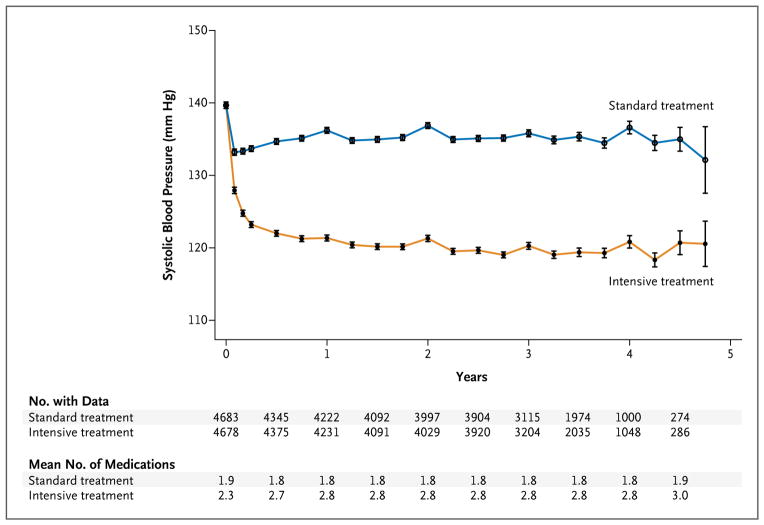
Methods: We randomly assigned 9361 persons with a systolic blood pressure of 130 mm Hg or higher and an increased cardiovascular risk, but without diabetes, to a systolic blood-pressure target of less than 120 mm Hg (intensive treatment) or a target of less than 140 mm Hg (standard treatment). The primary composite outcome was myocardial infarction, other acute coronary syndromes, stroke, heart failure, or death from cardiovascular causes.
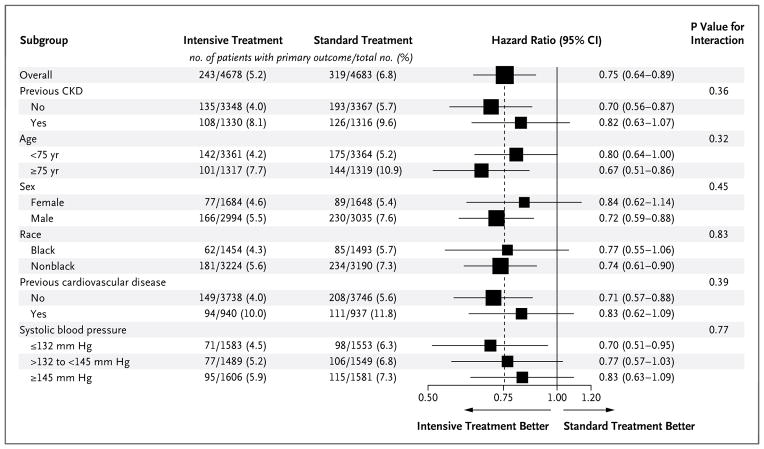
Results: At 1 year, the mean systolic blood pressure was 121.4 mm Hg in the intensive-treatment group and 136.2 mm Hg in the standard-treatment group. The intervention was stopped early after a median follow-up of 3.26 years owing to a significantly lower rate of the primary composite outcome in the intensive-treatment group than in the standard-treatment group (1.65% per year vs. 2.19% per year; hazard ratio with intensive treatment, 0.75; 95% confidence interval [CI], 0.64 to 0.89; P<0.001). All-cause mortality was also significantly lower in the intensive-treatment group (hazard ratio, 0.73; 95% CI, 0.60 to 0.90; P=0.003). Rates of serious adverse events of hypotension, syncope, electrolyte abnormalities, and acute kidney injury or failure, but not of injurious falls, were higher in the intensive-treatment group than in the standard-treatment group.
Conclusions: Among patients at high risk for cardiovascular events but without diabetes, targeting a systolic blood pressure of less than 120 mm Hg, as compared with less than 140 mm Hg, resulted in lower rates of fatal and nonfatal major cardiovascular events and death from any cause, although significantly higher rates of some adverse events were observed in the intensive-treatment group. (Funded by the National Institutes of Health; ClinicalTrials.gov number, NCT01206062.).
Figures


Comment in
-
A SPRINT to the Finish.N Engl J Med. 2015 Nov 26;373(22):2174-5. doi: 10.1056/NEJMe1513991. Epub 2015 Nov 9. N Engl J Med. 2015. PMID: 26551058 No abstract available.
-
Redefining Blood-Pressure Targets--SPRINT Starts the Marathon.N Engl J Med. 2015 Nov 26;373(22):2175-8. doi: 10.1056/NEJMe1513301. Epub 2015 Nov 9. N Engl J Med. 2015. PMID: 26551394 No abstract available.
-
Hypertension: Rest before blood pressure measurement: a lesson from SPRINT.Nat Rev Nephrol. 2016 Mar;12(3):127-8. doi: 10.1038/nrneph.2016.2. Epub 2016 Jan 25. Nat Rev Nephrol. 2016. PMID: 26804018 No abstract available.
-
ACP Journal Club. In patients with SBP ≥ 130 mm Hg and CV risk, intensive vs standard BP control reduced CV events and mortality.Ann Intern Med. 2016 Feb 16;164(4):JC15. doi: 10.7326/ACPJC-2016-164-4-015. Ann Intern Med. 2016. PMID: 26882300 No abstract available.
-
[A randomized trial of intensive versus standard blood pressure control].Semergen. 2016 Nov-Dec;42(8):e141-e143. doi: 10.1016/j.semerg.2015.12.009. Epub 2016 Mar 9. Semergen. 2016. PMID: 26968862 Spanish. No abstract available.
-
In hypertensive patients with elevated risk of cardiovascular disease, targeting systolic blood pressure to less than 120 mm Hg significantly reduces the rate of fatal and non-fatal cardiovascular events as well as death from any cause.Evid Based Med. 2016 Jun;21(3):101. doi: 10.1136/ebmed-2016-110397. Epub 2016 Mar 23. Evid Based Med. 2016. PMID: 27008978 No abstract available.
-
[Is lower still better? Reflections on Systolic Blood Pressure Intervention Trial study].Med Clin (Barc). 2016 Aug 5;147(3):127-9. doi: 10.1016/j.medcli.2016.02.012. Epub 2016 Mar 21. Med Clin (Barc). 2016. PMID: 27012671 Spanish. No abstract available.
-
How Does SPRINT (Systolic Blood Pressure Intervention Trial) Direct Hypertension Treatment Targets for CKD?Am J Kidney Dis. 2016 Jul;68(1):15-8. doi: 10.1053/j.ajkd.2016.02.045. Epub 2016 Mar 22. Am J Kidney Dis. 2016. PMID: 27012910 No abstract available.
-
A Randomized Trial of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2016 Jun 9;374(23):2294. doi: 10.1056/NEJMc1602668. N Engl J Med. 2016. PMID: 27276569 No abstract available.
-
A Randomized Trial of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2016 Jun 9;374(23):2290. doi: 10.1056/NEJMc1602668. N Engl J Med. 2016. PMID: 27276570 No abstract available.
-
A Randomized Trial of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2016 Jun 9;374(23):2290-1. doi: 10.1056/NEJMc1602668. N Engl J Med. 2016. PMID: 27276571 No abstract available.
-
A Randomized Trial of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2016 Jun 9;374(23):2291. doi: 10.1056/NEJMc1602668. N Engl J Med. 2016. PMID: 27276572 No abstract available.
-
A Randomized Trial of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2016 Jun 9;374(23):2291-2. doi: 10.1056/NEJMc1602668. N Engl J Med. 2016. PMID: 27276573 No abstract available.
-
A Randomized Trial of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2016 Jun 9;374(23):2292. doi: 10.1056/NEJMc1602668. N Engl J Med. 2016. PMID: 27276574 No abstract available.
-
A Randomized Trial of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2016 Jun 9;374(23):2292. doi: 10.1056/NEJMc1602668. N Engl J Med. 2016. PMID: 27276575 No abstract available.
-
A Randomized Trial of Intensive versus Standard Blood-Pressure Control.N Engl J Med. 2016 Jun 9;374(23):2293. doi: 10.1056/NEJMc1602668. N Engl J Med. 2016. PMID: 27276576 No abstract available.
-
Intensive lowering of blood pressure: Should we SPRINT?CMAJ. 2016 Oct 18;188(15):1067-1068. doi: 10.1503/cmaj.160147. Epub 2016 Jul 4. CMAJ. 2016. PMID: 27378462 Free PMC article. No abstract available.
-
Important practice lessons from the SPRINT study beyond the blood pressure goal: all well known and now confirmed.J Am Soc Hypertens. 2016 Aug;10(8):613-7. doi: 10.1016/j.jash.2016.06.002. Epub 2016 Jun 16. J Am Soc Hypertens. 2016. PMID: 27395782 No abstract available.
-
Lower is better in hypertension, but how low should blood pressure be targeted?J Am Soc Hypertens. 2016 Aug;10(8):621-2. doi: 10.1016/j.jash.2016.06.028. Epub 2016 Jun 18. J Am Soc Hypertens. 2016. PMID: 27436128 Free PMC article. No abstract available.
-
Intensive vs Standard Blood Pressure Control for Older Adults.JAMA. 2016 Nov 8;316(18):1922-1923. doi: 10.1001/jama.2016.14927. JAMA. 2016. PMID: 27825004 No abstract available.
-
How Low Should We Go With Blood Pressure?Circ Res. 2017 Jan 6;120(1):27-29. doi: 10.1161/CIRCRESAHA.116.309971. Circ Res. 2017. PMID: 28057786 No abstract available.
-
Is it premature to SPRINT?CMAJ. 2017 Feb 6;189(5):E217. doi: 10.1503/cmaj.732448. CMAJ. 2017. PMID: 28246267 Free PMC article. No abstract available.
-
The authors respond to "Is it premature to SPRINT?".CMAJ. 2017 Feb 6;189(5):E218. doi: 10.1503/cmaj.732527. CMAJ. 2017. PMID: 28246268 Free PMC article. No abstract available.
-
Der Hausarzt hält die Fäden in der Hand.MMW Fortschr Med. 2017 Oct;159(18):38. doi: 10.1007/s15006-017-0173-6. MMW Fortschr Med. 2017. PMID: 29071617 German. No abstract available.
-
Look before you SPRINT: look at the data and look at the consequences.Swiss Med Wkly. 2018 Jul 1;148:w14629. doi: 10.4414/smw.2018.14629. eCollection 2018. Swiss Med Wkly. 2018. PMID: 29964291 No abstract available.
References
-
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–23. - PubMed
-
- Franklin SS. Cardiovascular risks related to increased diastolic, systolic and pulse pressure: an epidemiologist’s point of view. Pathol Biol (Paris) 1999;47:594–603. - PubMed
-
- Franklin SS, Jacobs MJ, Wong ND, L’Italien GJ, Lapuerta P. Predominance of isolated systolic hypertension among middle-aged and elderly US hypertensives: analysis based on National Health and Nutrition Examination Survey (NHANES) III. Hypertension. 2001;37:869–74. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 Report. JAMA. 2003;289:2560–72. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1TR000433/TR/NCATS NIH HHS/United States
- UL1RR025752/RR/NCRR NIH HHS/United States
- UL1 TR000093/TR/NCATS NIH HHS/United States
- UL1TR000005/TR/NCATS NIH HHS/United States
- P30GM103337/GM/NIGMS NIH HHS/United States
- UL1 TR000050/TR/NCATS NIH HHS/United States
- UL1 RR025755/RR/NCRR NIH HHS/United States
- UL1 TR001085/TR/NCATS NIH HHS/United States
- UL1TR000439/TR/NCATS NIH HHS/United States
- UL1TR000064/TR/NCATS NIH HHS/United States
- UL1TR000075/TR/NCATS NIH HHS/United States
- P30 AG021332/AG/NIA NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- UL1TR000050/TR/NCATS NIH HHS/United States
- 9U54TR000017-06/TR/NCATS NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- HHSN268200900048C/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- UL1TR000445/TR/NCATS NIH HHS/United States
- HHSN268200900040C/HL/NHLBI NIH HHS/United States
- UL1TR000093/TR/NCATS NIH HHS/United States
- HHSN268200900046C/HL/NHLBI NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- UL1TR000002/TR/NCATS NIH HHS/United States
- UL1TR000073/TR/NCATS NIH HHS/United States
- UL1RR025755/RR/NCRR NIH HHS/United States
- UL1 TR000075/TR/NCATS NIH HHS/United States
- UL1RR025771/RR/NCRR NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- UL1 TR001064/TR/NCATS NIH HHS/United States
- UL1 RR025752/RR/NCRR NIH HHS/United States
- UL1TR000105-05/TR/NCATS NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- A-HL-13-002-001/HL/NHLBI NIH HHS/United States
- HHSN268200900049C/HL/NHLBI NIH HHS/United States
- HHSN268200900047C/HL/NHLBI NIH HHS/United States
- UL1 TR001427/TR/NCATS NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000073/TR/NCATS NIH HHS/United States
- UL1 TR000002/TR/NCATS NIH HHS/United States
- UL1 TR000105/TR/NCATS NIH HHS/United States
- UL1TR001064/TR/NCATS NIH HHS/United States
- UL1RR024134/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases