

Development of autoantibodies against muscle-specific FHL1 in severe inflammatory myopathies
- PMID: 26551678
- PMCID: PMC4665781
- DOI: 10.1172/JCI81031
Development of autoantibodies against muscle-specific FHL1 in severe inflammatory myopathies
Abstract
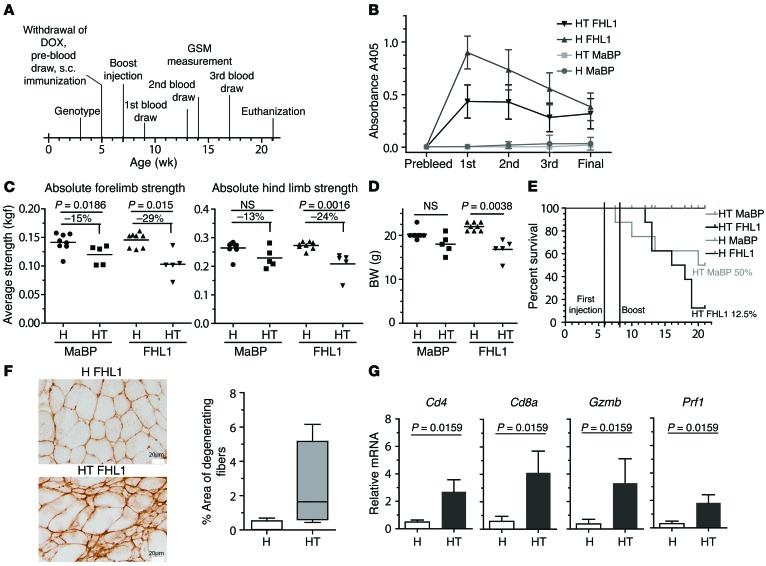
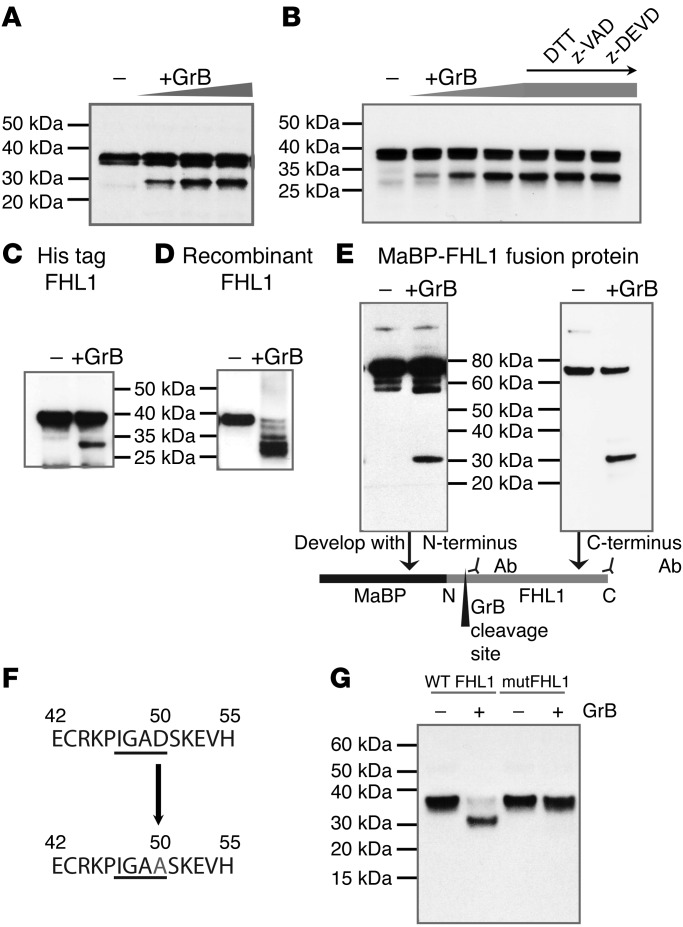
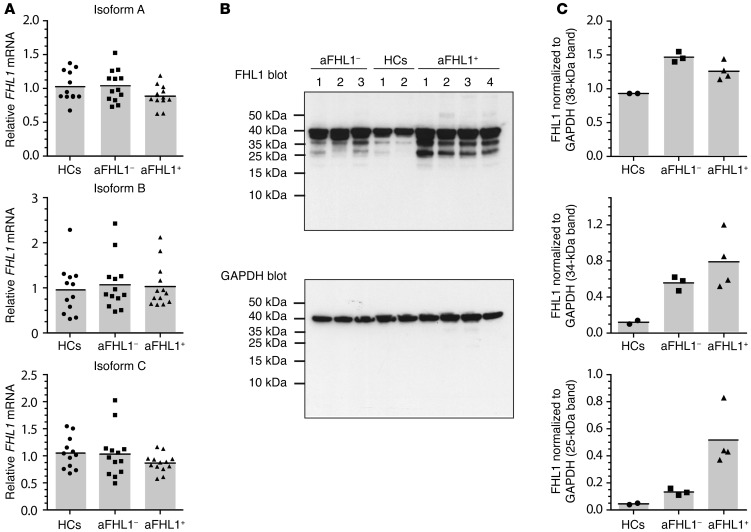
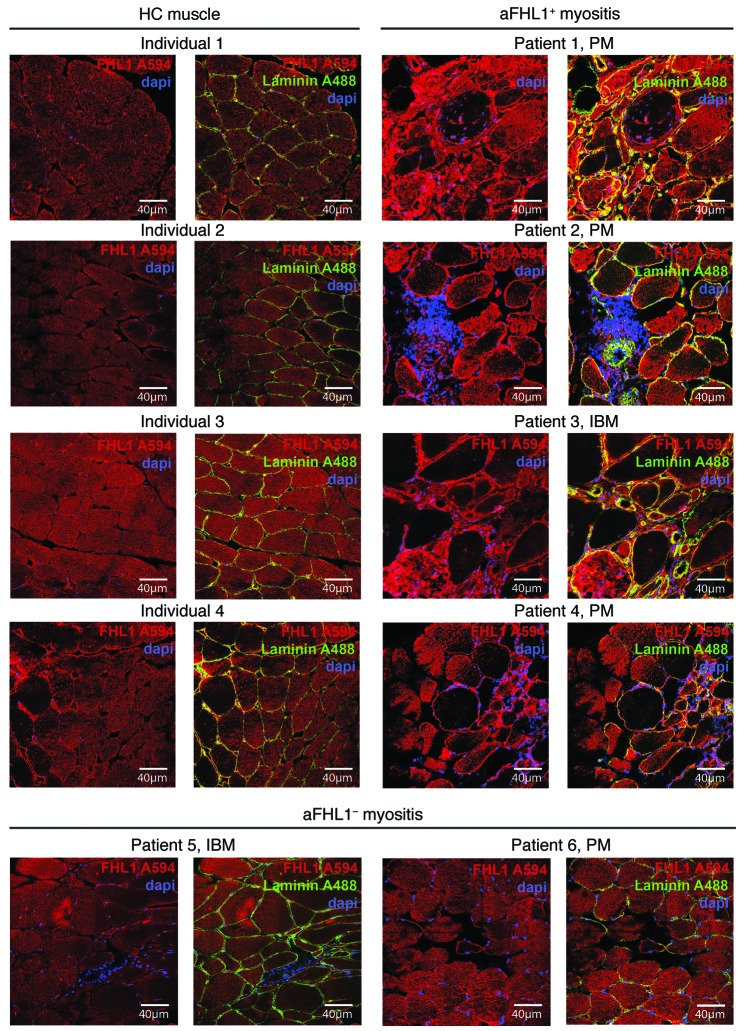
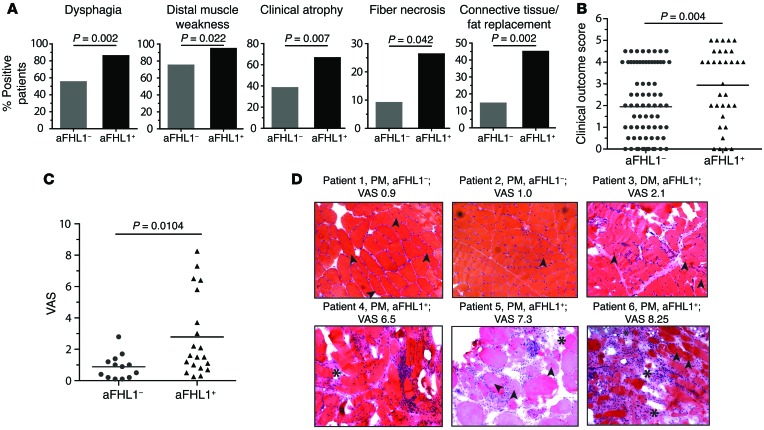
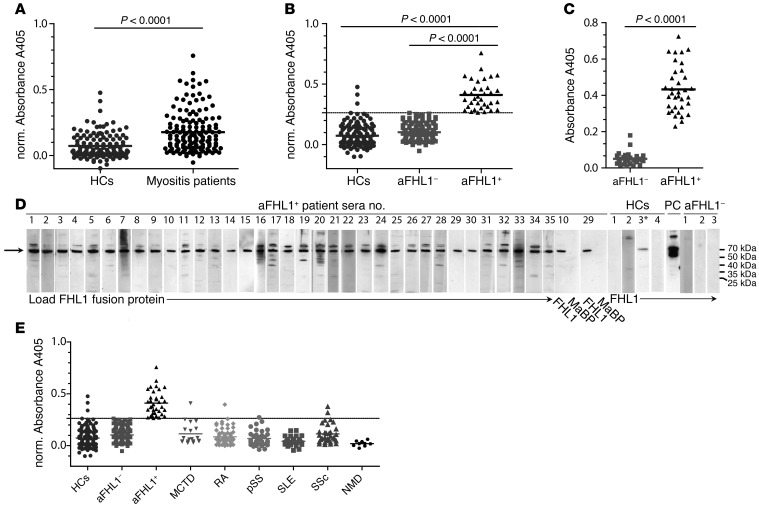
Mutations of the gene encoding four-and-a-half LIM domain 1 (FHL1) are the causative factor of several X-linked hereditary myopathies that are collectively termed FHL1-related myopathies. These disorders are characterized by severe muscle dysfunction and damage. Here, we have shown that patients with idiopathic inflammatory myopathies (IIMs) develop autoimmunity to FHL1, which is a muscle-specific protein. Anti-FHL1 autoantibodies were detected in 25% of IIM patients, while patients with other autoimmune diseases or muscular dystrophies were largely anti-FHL1 negative. Anti-FHL1 reactivity was predictive for muscle atrophy, dysphagia, pronounced muscle fiber damage, and vasculitis. FHL1 showed an altered expression pattern, with focal accumulation in the muscle fibers of autoantibody-positive patients compared with a homogeneous expression in anti-FHL1-negative patients and healthy controls. We determined that FHL1 is a target of the cytotoxic protease granzyme B, indicating that the generation of FHL1 fragments may initiate FHL1 autoimmunity. Moreover, immunization of myositis-prone mice with FHL1 aggravated muscle weakness and increased mortality, suggesting a direct link between anti-FHL1 responses and muscle damage. Together, our findings provide evidence that FHL1 may be involved in the pathogenesis not only of genetic FHL1-related myopathies but also of autoimmune IIM. Importantly, these results indicate that anti-FHL1 autoantibodies in peripheral blood have promising potential as a biomarker to identify a subset of severe IIM.
Figures
Comment in
-
Inflammatory myopathies: Anti-FHL1 antibodies linked to IIM.Nat Rev Rheumatol. 2016 Jan;12(1):2. doi: 10.1038/nrrheum.2015.168. Epub 2015 Nov 26. Nat Rev Rheumatol. 2016. PMID: 26607388 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
