

Benefits of an expanded use of plasma exchange for anti-neutrophil cytoplasmic antibody-associated vasculitis within a dedicated clinical service
- PMID: 26552432
- PMCID: PMC4640165
- DOI: 10.1186/s12891-015-0796-7
Benefits of an expanded use of plasma exchange for anti-neutrophil cytoplasmic antibody-associated vasculitis within a dedicated clinical service
Abstract
Background: Current recommendations for ANCA-associated vasculitis (AAV) support its management within a dedicated clinical service. Therapies for AAV are imperfect with many patients failing to achieve disease control and others experiencing disease relapse. Plasma exchange (PEX) may be beneficial especially when the kidney is involved.
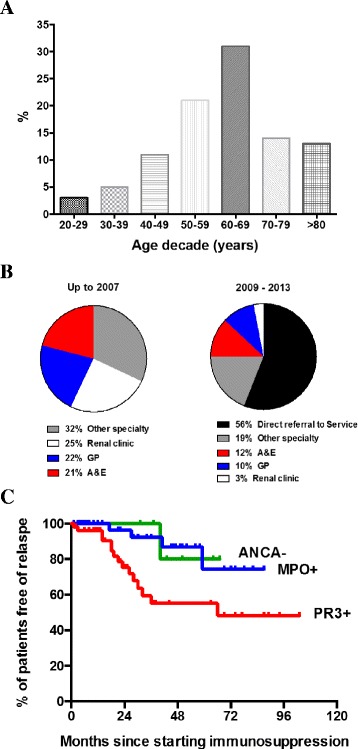
Methods: Within a new, dedicated service we retrospectively assessed, over a 6-year period, the benefits of PEX in two patient cohorts, discriminated by PEX treatment alone. Patients received PEX alongside standard of care if they fulfilled any of the following criteria: 1. serum creatinine >500 μmol/l or dialysis-requiring renal failure, 2. alveolar haemorrhage, 3. renal biopsy showing ≥30 % focal and necrotising lesions ± cellular crescents. Outcome measures included disease remission and relapse, cumulative immunosuppression, and morbidity and mortality.
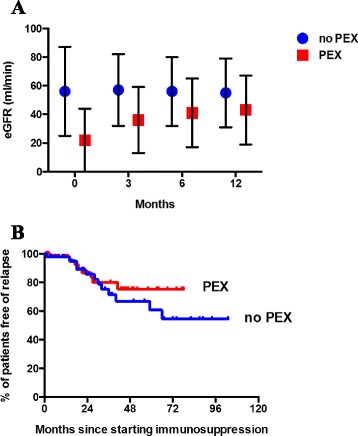
Results: Of 104 new patients, 58 patients received PEX at presentation, 46 did not. Cyclophosphamide and/or rituximab dosing was similar for both groups. Although patients receiving PEX had poorer renal function, a higher C-reactive protein and disease activity score at presentation disease remission rate was similar in both groups (no PEX vs. PEX: 96 % vs. 98 %). The PEX group entered remission quicker (no PEX vs. PEX: 3.9 ± 4.0 vs. 2.8 ± 1.3 months, p < 0.05), with a lower 3-month cumulative glucocorticoid dose (no PEX vs. PEX: 2.5 ± 0.4 vs. 2.3 ± 0.2 g, p < 0.001). Relapse was similar between groups but adverse events lower in the PEX group.
Conclusions: PEX may be of benefit in AAV. Larger, longer randomised controlled trials are now needed.
Figures
References
-
- Pagnoux C, Hogan SL, Chin H, Jennette JC, Falk RJ, Guillevin L, et al. Predictors of treatment resistance and relapse in antineutrophil cytoplasmic antibody-associated small-vessel vasculitis: comparison of two independent cohorts. Arthritis Rheum. 2008;58:2908–2918. doi: 10.1002/art.23800. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
