

Recurrent Laryngeal Nerve Liberations and Reconstructions: A Single Institution Experience
- PMID: 26552911
- PMCID: PMC4746230
- DOI: 10.1007/s00268-015-3305-0
Recurrent Laryngeal Nerve Liberations and Reconstructions: A Single Institution Experience
Abstract
Background: Recurrent laryngeal nerve (RLN) palsy rates vary from 0.5 to 10%, even 20% in thyroid cancer surgery. The aim of this paper was to present our experience with RLN liberations and reconstructions after various mechanisms of injury.
Methods: Patients were treated in our institution from year 2000 to 2015. First group (27 patients) had large benign goiters, locally advanced thyroid/parathyroid carcinomas, or incomplete previous surgery of malignant thyroid disease. Second group (5 patients) had reoperations due to RLN paralysis on laryngoscopy. Liberations and reconstructions of injured RLNs were performed.
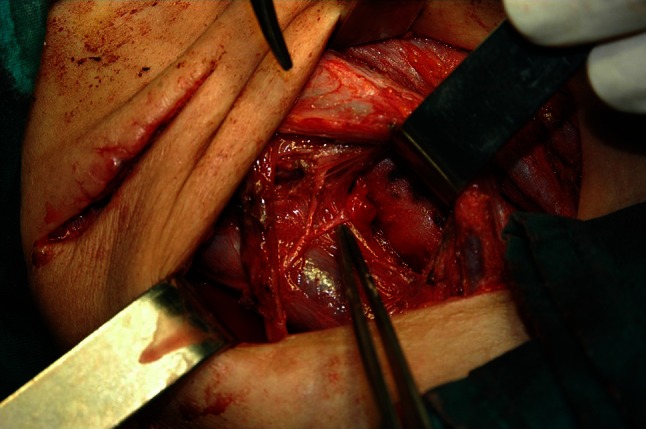
Results: Surgical exploration of central compartment enabled identification of the RLN injury mechanism. Liberations were performed in 11 patients, 2 months to 16 years after RLN injury, by removing misplaced ligations. Immediate or delayed (18 months to 23 years) RLN reconstructions were performed in 21 patients, by direct suture or ansa cervicalis-to-RLN anastomosis (ARA). RLN liberation provided complete voice recovery within 3 weeks in all patients. Patients with direct sutures had better phonation 1 month after reconstruction. Improved phonation was observed 2-6 months after ARA in 43% of patients.
Conclusions: Vocal cords do not regain normal movement once being paralyzed after RLN transection, but they restore tension during phonation by reconstruction. Nerve liberation is a useful method which enables patients with RLN paresis/paralysis a significant improvement in phonation, even complete voice recovery. Reinnervation of vocal cords, using one of the mentioned techniques, should be a standard in thyroid and parathyroid surgery, with aim to improve quality of patient's life.
Figures


Similar articles
-
Selective vagus-recurrent laryngeal nerve anastomosis in thyroidectomy with cancer invasion or iatrogenic transection.Langenbecks Arch Surg. 2020 Jun;405(4):461-468. doi: 10.1007/s00423-020-01906-y. Epub 2020 Jun 6. Langenbecks Arch Surg. 2020. PMID: 32504208
-
Surgical Methods and Experiences of Surgeons did not Significantly Affect the Recovery in Phonation Following Reconstruction of the Recurrent Laryngeal Nerve.World J Surg. 2016 Dec;40(12):2948-2955. doi: 10.1007/s00268-016-3634-7. World J Surg. 2016. PMID: 27431320 Free PMC article.
-
The role of ansa-to-recurrent-laryngeal nerve anastomosis in operations for thyroid cancer.Eur J Surg. 1998 Dec;164(12):927-33. doi: 10.1080/110241598750005093. Eur J Surg. 1998. PMID: 10029388
-
Immediate Intraoperative Repair of the Recurrent Laryngeal Nerve in Thyroid Surgery.Laryngoscope. 2021 Jun;131(6):1429-1435. doi: 10.1002/lary.29204. Epub 2020 Oct 29. Laryngoscope. 2021. PMID: 33118630 Review.
-
Laryngeal Reinnervation: The History and Where We Stand Now.Adv Otorhinolaryngol. 2020;85:98-111. doi: 10.1159/000456688. Epub 2020 Nov 9. Adv Otorhinolaryngol. 2020. PMID: 33166981 Review.
Cited by
-
The Role of Primary Repair of the Recurrent Laryngeal Nerve during Thyroid/Parathyroid Surgery in Vocal Outcomes-A Systematic Review.J Clin Med. 2023 Feb 3;12(3):1212. doi: 10.3390/jcm12031212. J Clin Med. 2023. PMID: 36769864 Free PMC article. Review.
-
Selective vagus-recurrent laryngeal nerve anastomosis in thyroidectomy with cancer invasion or iatrogenic transection.Langenbecks Arch Surg. 2020 Jun;405(4):461-468. doi: 10.1007/s00423-020-01906-y. Epub 2020 Jun 6. Langenbecks Arch Surg. 2020. PMID: 32504208
-
A narrative review of current therapies in unilateral recurrent laryngeal nerve injury caused by thyroid surgery.Gland Surg. 2022 Jan;11(1):270-278. doi: 10.21037/gs-21-708. Gland Surg. 2022. PMID: 35242688 Free PMC article. Review.
-
Advances in the assessment of cosmetic outcomes, sensory alteration in surgical areas, and health-related quality of life of endoscopic thyroidectomy.World J Surg Oncol. 2024 Feb 13;22(1):52. doi: 10.1186/s12957-024-03307-7. World J Surg Oncol. 2024. PMID: 38347606 Free PMC article. Review.
-
Long-term quality of voice is usually acceptable after initial hoarseness caused by a thyroidectomy or a parathyroidectomy.Gland Surg. 2019 Jun;8(3):226-236. doi: 10.21037/gs.2018.09.02. Gland Surg. 2019. PMID: 31328101 Free PMC article.
References
-
- Levin KE, Clark AH, Duh QY, et al. Reoperative thyroid surgery. Surgery. 1992;111:604–609. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
