

Interval analysis of interictal EEG: pathology of the alpha rhythm in focal epilepsy
- PMID: 26553287
- PMCID: PMC4639771
- DOI: 10.1038/srep16230
Interval analysis of interictal EEG: pathology of the alpha rhythm in focal epilepsy
Abstract
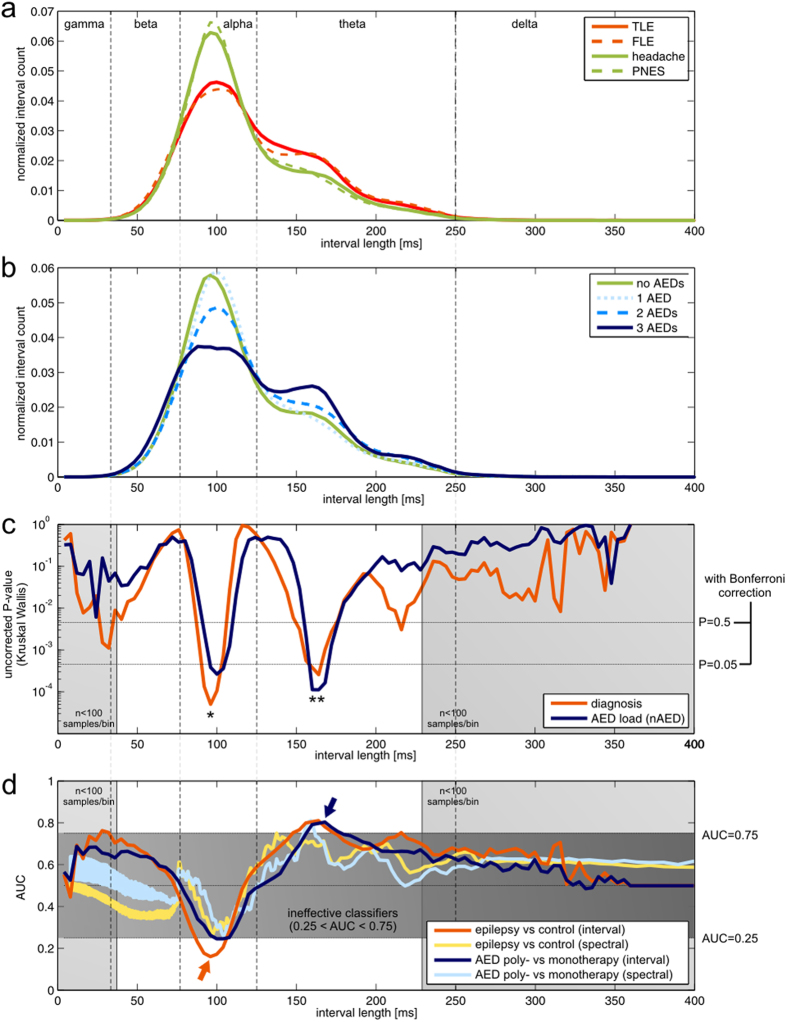
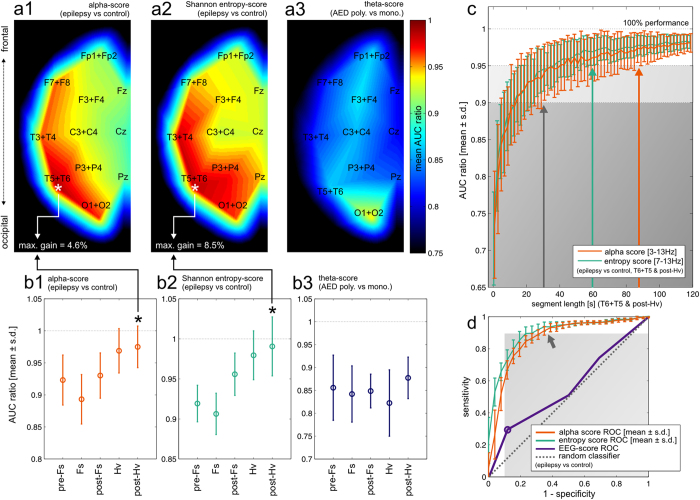
The contemporary use of interictal scalp electroencephalography (EEG) in the context of focal epilepsy workup relies on the visual identification of interictal epileptiform discharges. The high-specificity performance of this marker comes, however, at a cost of only moderate sensitivity. Zero-crossing interval analysis is an alternative to Fourier analysis for the assessment of the rhythmic component of EEG signals. We applied this method to standard EEG recordings of 78 patients divided into 4 subgroups: temporal lobe epilepsy (TLE), frontal lobe epilepsy (FLE), psychogenic nonepileptic seizures (PNES) and nonepileptic patients with headache. Interval-analysis based markers were capable of effectively discriminating patients with epilepsy from those in control subgroups (AUC~0.8) with diagnostic sensitivity potentially exceeding that of visual analysis. The identified putative epilepsy-specific markers were sensitive to the properties of the alpha rhythm and displayed weak or non-significant dependences on the number of antiepileptic drugs (AEDs) taken by the patients. Significant AED-related effects were concentrated in the theta interval range and an associated marker allowed for identification of patients on AED polytherapy (AUC~0.9). Interval analysis may thus, in perspective, increase the diagnostic yield of interictal scalp EEG. Our findings point to the possible existence of alpha rhythm abnormalities in patients with epilepsy.
Figures
References
-
- Noachtar S. & Rémi J. The role of EEG in epilepsy: a critical review. Epilepsy Behav. 15, 22–33 (2009). - PubMed
-
- Bodde N. M. G. et al. Psychogenic non-epileptic seizures—diagnostic issues: a critical review. Clin. Neurol. Neurosurg. 111, 1–9 (2009). - PubMed
-
- Stoller A. Slowing of the Alpha-Rhythm of the Electro-Encephalogram and its Association with Mental Deterioration and Epilepsy. Br. J. Psychiatry 95, 972–984 (1949). - PubMed
-
- Benbadis S. R. & Tatum W. O. Overintepretation of EEGs and misdiagnosis of epilepsy. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 20, 42–44 (2003). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
