

Defining Appropriate Use of Proton-Pump Inhibitors Among Medical Inpatients
- PMID: 26553337
- PMCID: PMC4803704
- DOI: 10.1007/s11606-015-3536-7
Defining Appropriate Use of Proton-Pump Inhibitors Among Medical Inpatients
Abstract
Background: Proton-pump inhibitors (PPIs) are commonly used among medical inpatients, both for prophylaxis against upper gastrointestinal bleeding (UGIB) and continuation of outpatient use. While PPIs reduce the risk of UGIB, they also appear to increase the risk of hospital-acquired pneumonia (HAP) and Clostridium difficile infection (CDI). Depending upon the underlying risks of these conditions and the changes in those risks with PPIs, use of proton-pump inhibitors may lead to a net benefit or net harm among medical inpatients.
Objective: We aimed to determine the net impact of PPIs on hospital mortality among medical inpatients.
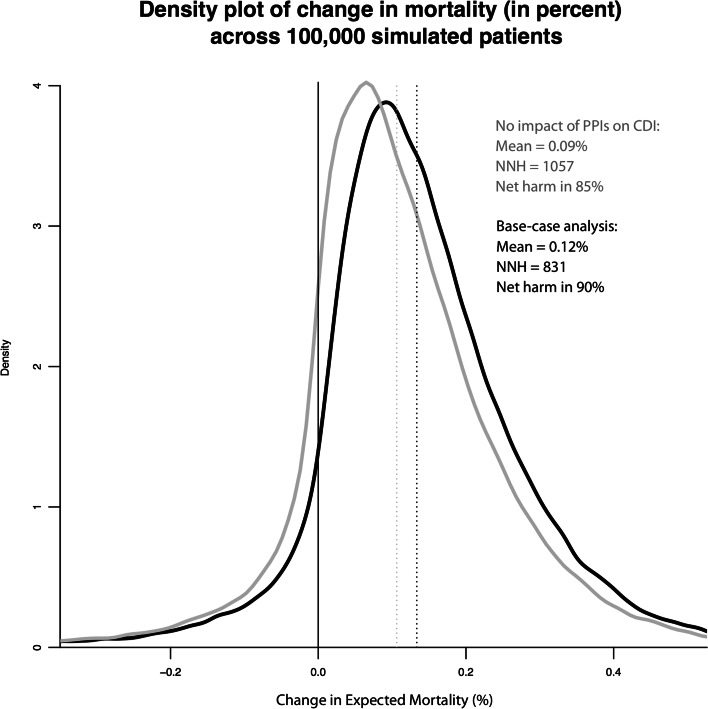
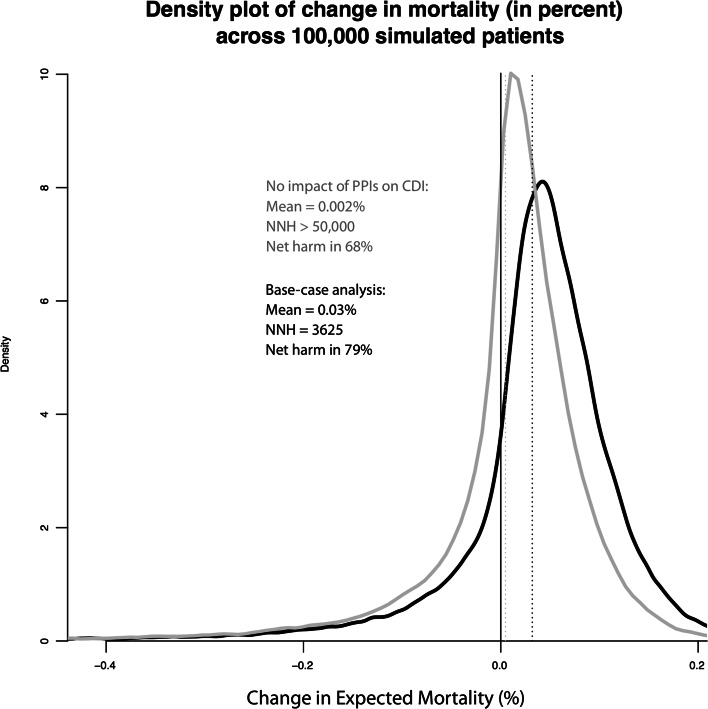
Design: A microsimulation model, using literature-derived estimates of the risks of UGIB, HAP, and CDI among medical inpatients, along with the changes in risk associated with PPI use for each of these outcomes. The primary outcome was change in inpatient mortality.
Participants: Simulated general medical inpatients outside the intensive care unit (ICU).
Main measure: Change in overall mortality during hospitalization.
Key results: New initiation of PPI therapy led to an increase in hospital mortality in about 90% of simulated patients. Continuation of outpatient PPI therapy on admission led to net increase in hospital mortality in 79% of simulated patients. Results were robust to both one-way and multivariate sensitivity analyses, with net harm occurring in at least two-thirds of patients in all scenarios.
Conclusions: For the majority of medical inpatients outside the ICU, use of PPIs likely leads to a net increase in hospital mortality. Even in patients at particularly high risk of UGIB, only those at the very lowest risk of HCAP and CDI should be considered for prophylactic PPI use. Continuation of outpatient PPIs may also increase expected hospital mortality. Apart from patients with active UGIB, use of PPIs in hospitalized patients should be discouraged.
Keywords: hospital medicine; medical decision making; modeling; simulation.
Conflict of interest statement
Compliance with Ethical Standards Conflicts of interest The authors declare that they do not have a conflict of interest.
Figures
Comment in
-
Reconsidering a Common Practice: In-Hospital Use of PPIs.J Gen Intern Med. 2016 Apr;31(4):361-2. doi: 10.1007/s11606-015-3565-2. J Gen Intern Med. 2016. PMID: 26693727 Free PMC article. No abstract available.
Similar articles
-
Proton pump inhibitors increase the risk for hospital-acquired Clostridium difficile infection in critically ill patients.Crit Care. 2014 Dec 24;18(6):714. doi: 10.1186/s13054-014-0714-7. Crit Care. 2014. PMID: 25540023 Free PMC article.
-
Histamine-2 receptor antagonists vs proton pump inhibitors on gastrointestinal tract hemorrhage and infectious complications in the intensive care unit.JAMA Intern Med. 2014 Apr;174(4):564-74. doi: 10.1001/jamainternmed.2013.14673. JAMA Intern Med. 2014. PMID: 24535015
-
Proton pump inhibitors and risk for recurrent Clostridium difficile infection among inpatients.Am J Gastroenterol. 2013 Nov;108(11):1794-801. doi: 10.1038/ajg.2013.333. Epub 2013 Sep 24. Am J Gastroenterol. 2013. PMID: 24060760 Free PMC article.
-
Optimizing proton pump inhibitor therapy for treatment of nonvariceal upper gastrointestinal bleeding.Am J Health Syst Pharm. 2017 Feb 1;74(3):109-116. doi: 10.2146/ajhp151032. Am J Health Syst Pharm. 2017. PMID: 28122752 Review.
-
Updated meta-analysis of controlled observational studies: proton-pump inhibitors and risk of Clostridium difficile infection.J Hosp Infect. 2018 Jan;98(1):4-13. doi: 10.1016/j.jhin.2017.08.017. Epub 2017 Aug 24. J Hosp Infect. 2018. PMID: 28842261 Review.
Cited by
-
Empiricism as Change Agent.J Gen Intern Med. 2016 Apr;31(4):359-60. doi: 10.1007/s11606-016-3595-4. J Gen Intern Med. 2016. PMID: 26831307 Free PMC article. No abstract available.
-
A Nomogram for Individualized Prediction of Stress-Related Gastrointestinal Bleeding in Critically Ill Patients with Primary Intracerebral Hemorrhage.Neuropsychiatr Dis Treat. 2022 Feb 9;18:221-229. doi: 10.2147/NDT.S342861. eCollection 2022. Neuropsychiatr Dis Treat. 2022. PMID: 35177906 Free PMC article.
-
Outcomes From a Pharmacist - led Proton Pump Inhibitor Stewardship Program at a Single Institution.Hosp Pharm. 2018 Feb;53(1):59-67. doi: 10.1177/0018578717747192. Epub 2017 Dec 13. Hosp Pharm. 2018. PMID: 29434389 Free PMC article.
-
Use of proton pump inhibitors and mortality after hip fracture in a nationwide study.Osteoporos Int. 2017 May;28(5):1587-1595. doi: 10.1007/s00198-017-3910-x. Epub 2017 Jan 12. Osteoporos Int. 2017. PMID: 28083667
-
Reducing Inappropriate Proton Pump Inhibitors Use for Stress Ulcer Prophylaxis in Hospitalized Patients: Systematic Review of De-Implementation Studies.J Gen Intern Med. 2021 Jul;36(7):2065-2073. doi: 10.1007/s11606-020-06425-6. Epub 2021 Feb 2. J Gen Intern Med. 2021. PMID: 33532958 Free PMC article.
References
-
- Nardino RJ, Vender RJ, Herbert PN. Overuse of acid-suppressive therapy in hospitalized patients. Am J Gastroenterol. 2000;95(11):3118–3122. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
