

Does a Positive Axillary Lymph Node Needle Biopsy Result Predict the Need for an Axillary Lymph Node Dissection in Clinically Node-Negative Breast Cancer Patients in the ACOSOG Z0011 Era?
- PMID: 26553439
- PMCID: PMC4775411
- DOI: 10.1245/s10434-015-4944-y
Does a Positive Axillary Lymph Node Needle Biopsy Result Predict the Need for an Axillary Lymph Node Dissection in Clinically Node-Negative Breast Cancer Patients in the ACOSOG Z0011 Era?
Abstract
Background: American College of Surgeons Oncology Group (ACOSOG) Z0011 defined clinical node negativity by physical examination alone. Although axillary ultrasound with biopsy has a positive predictive value for lymph node (LN) metastases approaching 100 %, it may not appropriately identify clinically node-negative women with ≥3 positive LNs who require axillary lymph node dissection (ALND). We sought to identify the total number of positive LNs in women presenting with cT1-2N0 breast carcinoma with a positive preoperative LN biopsy to evaluate the potential for overtreatment when ALND is performed on the basis of a positive needle biopsy in patients who otherwise meet ACOSOG Z0011 eligibility criteria.
Methods: Patients with cT1-2N0 breast cancer by physical examination with a positive preoperative LN biopsy were identified from a prospective institutional database. Clinicopathologic characteristics and axillary imaging results were compared between women with 1 to 2 total positive LNs and ≥3 total positive LNs.
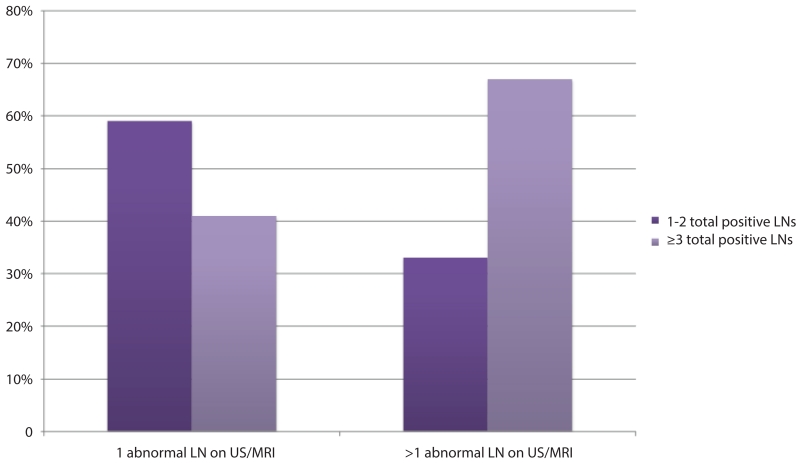
Results: Between May 2006 and December 2013, a total of 141 women with cT1-2N0 breast cancer had abnormal axillary imaging and a preoperative positive LN biopsy (median patient age 51 years, median tumor size 2.4 cm, 86 % ductal histology, 79 % estrogen receptor positive). Sixty-six women (47 %) had 1 to 2 total positive LNs, and 75 (53 %) had ≥3 total positive LNs. Women with ≥3 total positive LNs had larger tumors (2.4 vs. 2.2 cm, p = 0.03), fewer tumors with ductal histology (79 vs. 94 %, p = 0.01), more lymphovascular invasion (80 vs. 61 %, p = 0.01), and higher median body mass index (29.2 vs. 27.1 kg/m(2), p = 0.04). Having >1 abnormal LN on axillary imaging was significantly associated with having ≥3 total positive LNs at final pathology (68 vs. 43 %, p = 0.003).
Conclusions: Axillary imaging with preoperative LN biopsy does not accurately discriminate low- versus high-volume nodal disease in clinically node-negative patients.
Figures
References
-
- Giuliano AE, McCall L, Beitsch P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg. 2010;252(3):426–32. discussion 32-3. - PMC - PubMed
-
- Sola M, Alberro JA, Fraile M, et al. Complete axillary lymph node dissection versus clinical follow-up in breast cancer patients with sentinel node micrometastasis: final results from the multicenter clinical trial AATRM 048/13/2000. Ann Surg Oncol. 2013;20(1):120–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
