

Fibrosis is a common outcome following total knee arthroplasty
- PMID: 26553967
- PMCID: PMC4639721
- DOI: 10.1038/srep16469
Fibrosis is a common outcome following total knee arthroplasty
Abstract
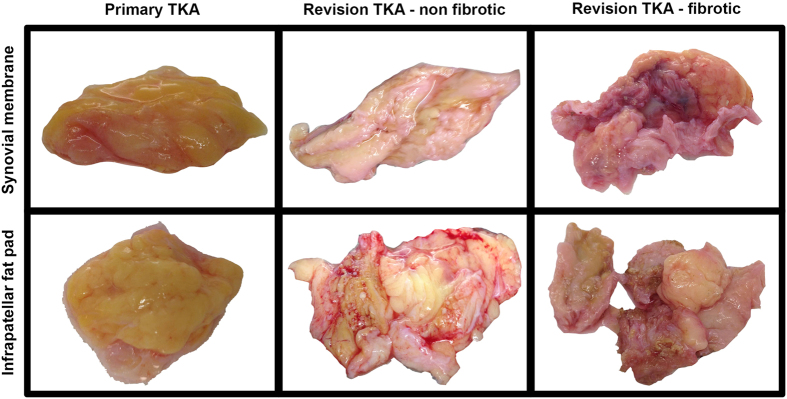
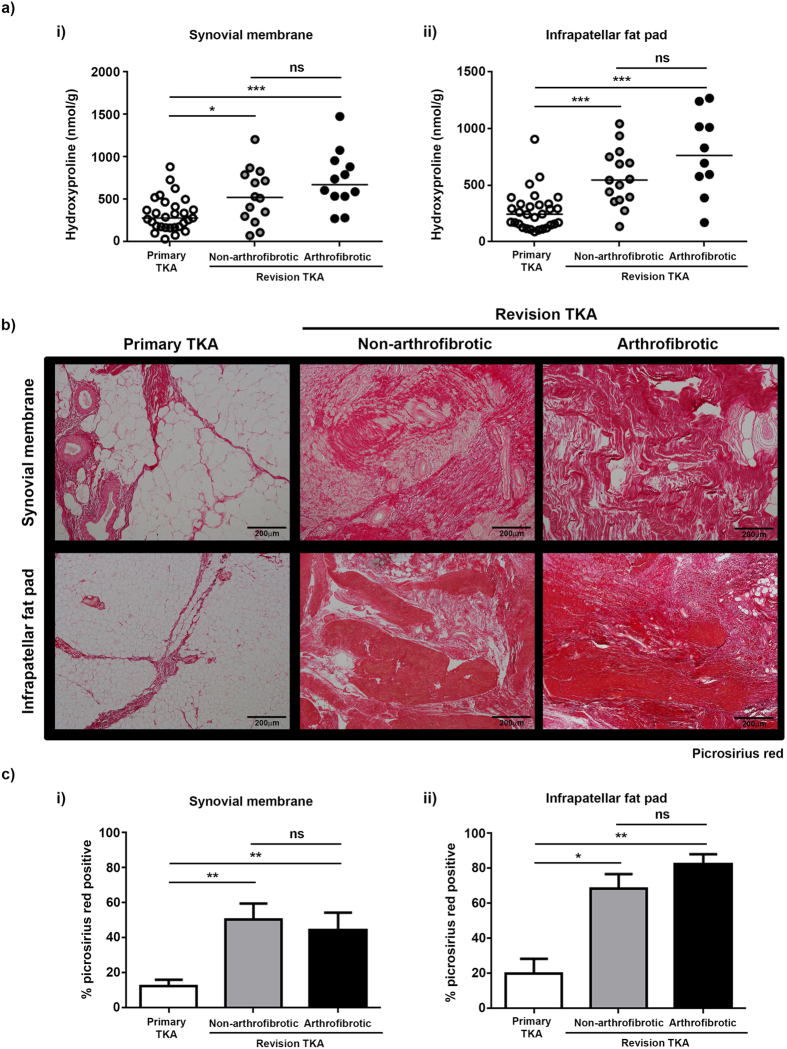
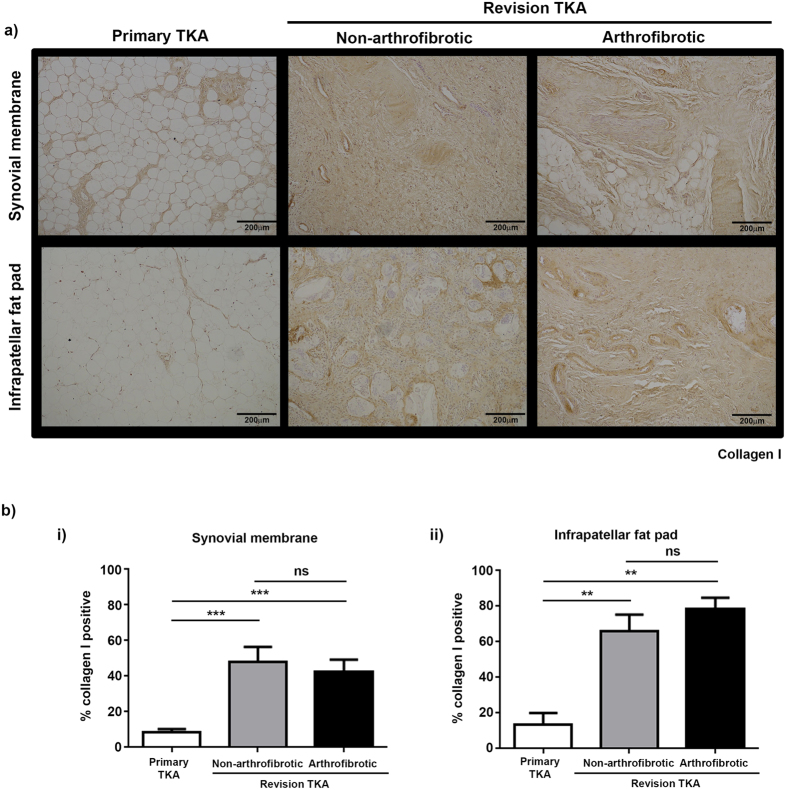
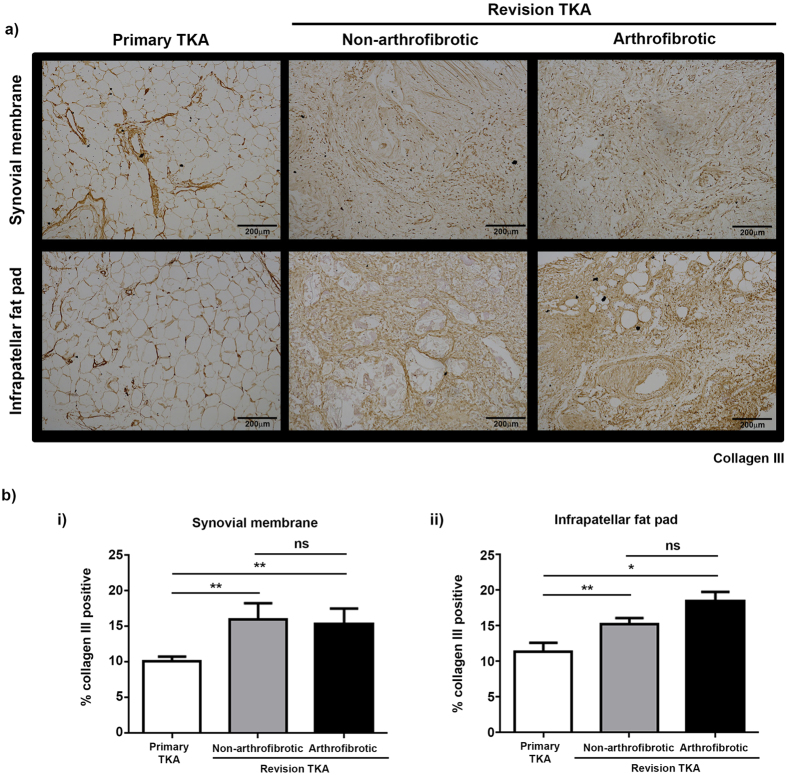
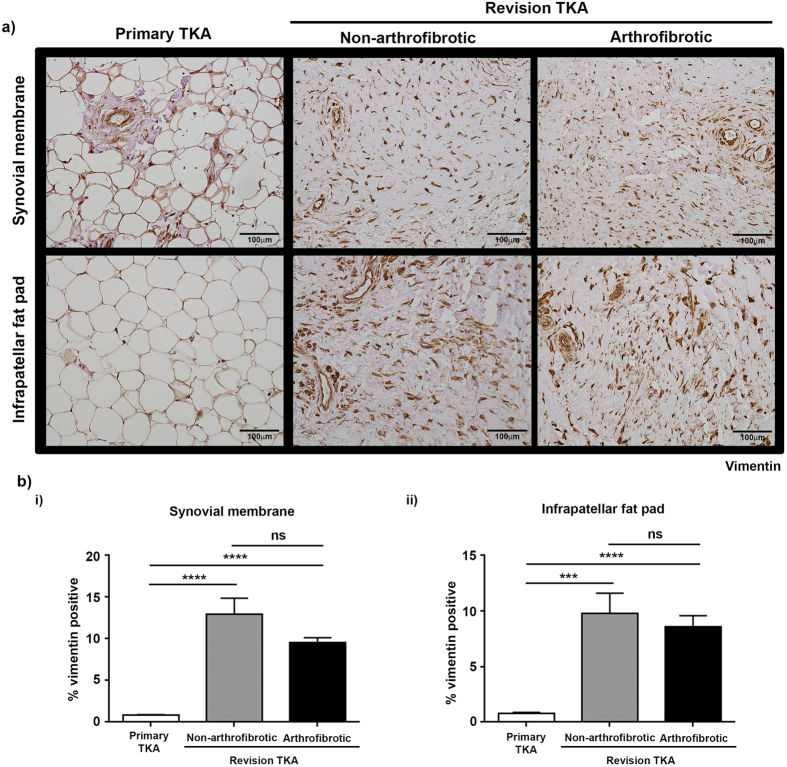
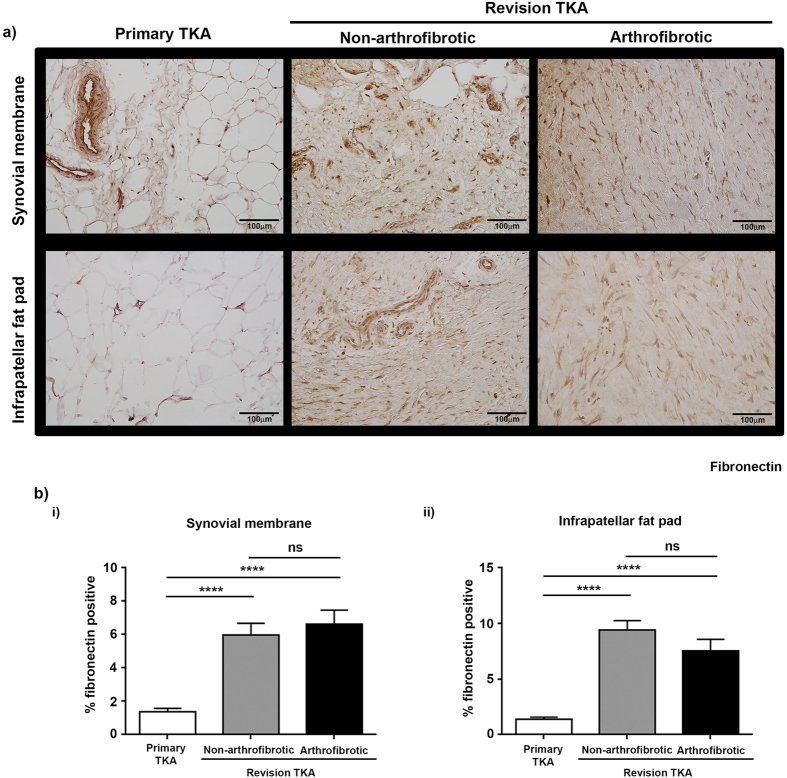
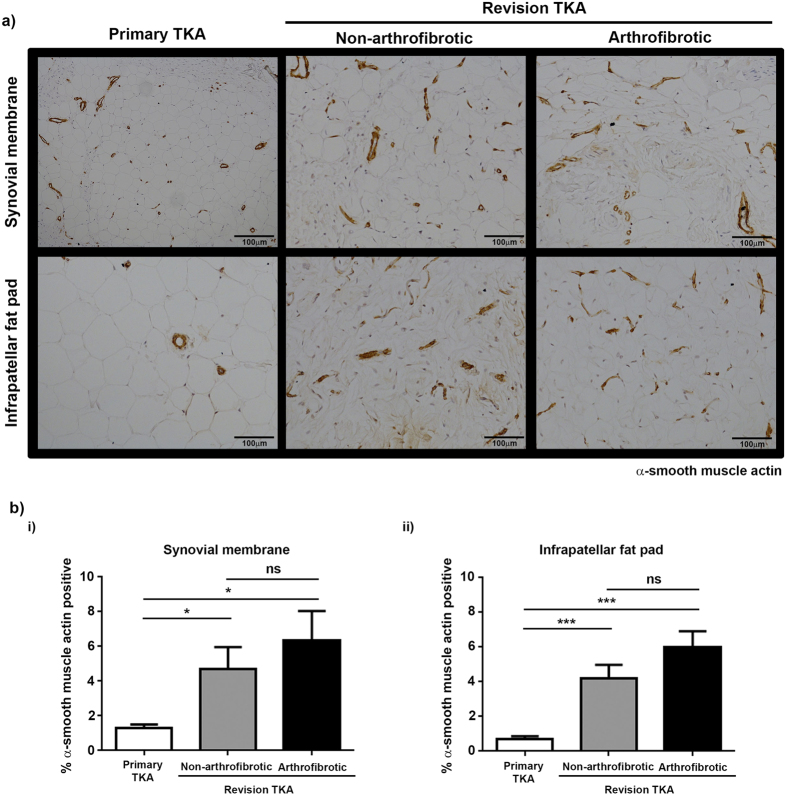
Total knee arthroplasty (TKA) is one of the most successful orthopaedic procedures that alleviates pain and restores function in patients with degenerative knee joint diseases. Arthrofibrosis, abnormal scarring in which dense fibrous tissue prevents normal range of motion, develops in ~3-10% of TKA patients. No prophylactic intervention is available and treatment is restricted to aggressive physiotherapy or revision surgery. Tissue was collected from patients undergoing primary (n = 30) or revision (n = 27) TKA. Revision patients were stratified as non-arthrofibrotic and arthrofibrotic. Tissue was macroscopically and histologically compared to improve our understanding of the pathophysiology of arthrofibrosis. Macroscopically, tissue from primary TKA presents as homogenous, fatty tissue whereas tissue from revision TKA presents as dense, pigmented tissue. Histologically, there was dramatic tissue remodelling, increased collagen deposition and increased (myo)fibroblast staining in tissue from revision TKA. Significantly, tissue architecture was similar between revision patients regardless of clinically diagnosis. There are significant differences in architecture and composition of tissue from revision TKA over primary TKA. Surprisingly, whether revision TKA were clinically diagnosed as arthrofibrotic or non-arthrofibrotic there were still significant differences in fibrotic markers compared to primary TKA suggesting an ongoing fibrotic process in all revision knees.
Conflict of interest statement
NB has a knee consultancy contract with Stryker.
Figures
References
-
- Baker P. N. et al. Patient satisfaction with total knee replacement cannot be predicted from pre-operative variables alone: A cohort study from the National Joint Registry for England and Wales. Bone Joint J 95-B, 1359–1365 (2013). - PubMed
-
- Carr A. J. et al. Knee replacement. Lancet 379, 1331–1340 (2012). - PubMed
-
- Gandhi R. et al. Predictive risk factors for stiff knees in total knee arthroplasty. J arthroplasty 21, 46–52 (2006). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
